Barriers of Implementing E-Health in Developing Countries: A Case Study: Syria
2023-08-19 | Volume 1 Issue 2 - Volume 1 | Review Articles | Mouhamad Kawas | Bassel AlKhatibAbstract
Advancements in technology have significantly influenced members’ lives, like e-Health implementation, which brings numerous benefits to the healthcare sector, including cost reduction. However, developing countries are facing challenges in adopting e-health solutions, including electronic health record (EHR) systems. This research conducts a meta-analysis, focusing on the sustainable adoption of e-Health in developing countries, using Syria as a case study. The study analyzes 20 peer-reviewed articles collected from online databases. The thematic analysis identifies four interconnected themes: social, economic, cultural, and organizational factors influencing the successful adoption of e-health in developing countries like Syria. Understanding these factors is vital for devising effective strategies to promote the sustainable integration of e-Health technologies in the healthcare systems of developing nations.
Keywords : E-Health, EHR, Telemedicine, Medical Informatics, Sustainability.
INTRODUCTION
Growth and technological advances have immensely contributed to streamlining modern living. Almost every aspect of human life relies on the benefits of modern technology. The adoption of technology in the healthcare system is referred to as e-Health. According to Elharish et al [1], e-Health is the delivery of healthcare using modern electronic information and communication technologies. Healthcare services provided through electronic health include physical and psychological diagnosis and treatment, telepathology, vital sign monitoring, and teleconsultation, and the adoption of e-Health benefits healthcare practitioners and patients. Benefits of E-Health include saving time, reducing human errors, reducing healthcare costs, and giving patients insight into their health. The benefits of e-Health adoption have been seen in different regions worldwide. Despite the perceived benefits, developing countries show a go-slow in adopting e-Health. Prior studies explain the latter scenario from the funding and cost constraints perspective. However, other factors have contributed to the sustainable adoption of e-Health technology in developing countries. To facilitate swift and sustainable adoption of e-Health in developing countries, involved stakeholders should understand the connection between social, economic, and political factors challenging e-Health adoption in developing countries.
This research will expound the discussion on factors affecting the sustainable adoption of e-Health in developing countries using Syria as a case study. A meta-analysis of the current situation in Syria was conducted using online peer-reviewed databases such as Google Scholar, PMC, and PubMed. As mentioned earlier, the current study explains the slow adoption of e-Health in developing countries. The latter approach leaves many gaps in explaining the influence of social, political, and cultural factors impacting the adoption of e-Health in Syria. By addressing the research gap, the study will enhance the process of adapting e-Health in Syria and other developing countries. Sustainable adoption of e-Health requires a region to evaluate its capability and feasibility of the intended changes. However, external and internal factors within a jurisdiction compromise the latter moves. Developing the country’s economic, social, cultural, and organizational traits are among the most conspicuous factors affecting the sustainable adoption of e-Health. The situation in Syria is far worse than in many developing countries in the Middle East. The Syrian war has weakened the country’s ICT infrastructure, and the interplay between various cultural, economic, and war contributions has led to the unsustainable adoption of e-Health in Syria. Understanding factors compromising e-Health adoption in Syria gives the government a clear picture of evidence-based measures for improving its healthcare system.
The Syrian government has emphasized a decentralized healthcare system that focuses on providing primary healthcare at the village, district, and provincial levels. Irrespective of the measures embraced to streamline healthcare provision in Syria, the progressive wars in the region have seen a 60% decline in Syrian health care services. In addition to causing a decline in Syria`s population, the war in Syria is responsible for destroying healthcare infrastructure and, consequently, unsustainable adoption of e-Health. Medical facilities’ destruction has led to shortages of medications and medical supplies. In a report by the International Rescue Committee (IRC), Syria has a total of 507 hospitals (114 public hospitals and 393 private hospitals), which are distributed between cities unevenly. The latter statistics are grounded on attacks directed on healthcare facilities. According to Allah ham et al, (2022) [2]. Berlin-headquartered Syrian archive has documented videos of 412 separate attacks against a total of 270 medical facilities between 2011 and 2020. The progress of the Syrian war has increased healthcare disparities in the region, with an average of 706 persons per bed in 2020 compared to 734 persons per bed in 2011. The current situation in Syria requires immediate action, following that only 64% of hospitals and 52% of the region’s health care centers are functional [2]. Direct attacks on Syria`s health facilities and practitioners have seen a significant drop in healthcare practitioners. According to Karasapan (2016) [3], 70% of Syria’s healthcare providers have fled the country, with substantial cities experiencing mass migration of physicians. Aleppo, one of the major cities in Syrian, had 6000 physicians before the war, and by 2013 only 250 remained in the city. The deteriorating state of Syria`s health sector is also founded on reduced government spending on health as a percentage of GDP. According to Allahham et al, (2022) [2], Syria`s government spending on health reduced from 4.9% in 2005 to 3.4 % in 2010 and continued to reach less than half of the 2011 percentage.
Article Statement: The slow adoption of e-Health technology in developing countries is a multifaceted issue requiring responsible stakeholders to devise and resolve practical measures.
LITERATURE REVIEW
Lack of Awareness
The rate of technology acceptance varies with region and community members’ attitudes towards the technology. Cultural, economic, and social factors define innovation adoption rates resulting in five categories (innovators, early adopters, early majority, late majority, and laggards) of innovation [4]. Developed countries comprise early adopters and innovators. While innovators are motivated to accept trends in technology as soon as they emerge and appreciate technological changes, early adopters adopt new technology to achieve revolutionary changes and gain a competitive advantage. On the other hand, the early majority embrace technological changes to improve productivity. Syria and many developing countries fall into the laggards and late majority category. The latter categories are skeptical about innovative technology and are geared towards maintaining the current status quo. Cultural and organizational traits in Middle East countries explain the region’s unsustainable adoption of e-Health technology. Alajlani & Clarke [5] conducted case study research in Syria and Jordan to investigate cultural factors affecting the sustainable adoption of e-Health in the two regions. The study gathered data from key stakeholders in Syria and Jordan’s healthcare sector. Interviews and questionnaires were employed for a study population comprising 100 participants (50 from each country) and 45 professional participants (22 from Jordan and 23 from Syria). The study accessed the professional practitioners using face-to-face semi-structured interviews. The study aimed to investigate demographic traits in the two regions and identify factors likely to compromise e-Health adoption.
A thematic analysis revealed three interconnected themes; poor infrastructure, poor funding, and lack of technology training as significant factors leading to the slow adoption of e-Health. It was noted that Jordan was ahead of Syria in adopting e-Health. This was supported by the fact that Jordan started using e-Health technology way of Syria. Even though the two countries had problems funding e-Health programs, respondents from Syria did not perceive funding as a barrier to e-Health implementation [5]. Regardless of the noted difference, resistance from doctors and patients was a major factor affecting the sustainable development of e-Health. Lack of training and exposure to e-Health affected Syrian health professionals more than in Jordan. The latter findings align with the categories of innovators highlighted in the introduction. Syria falls in the laggard category of innovators, which explains why its health practitioners and patients display a go-slow in accepting e-Health.
Reform Challenges
Rapid development in information and communication technology requires community members and affected individuals to stipulate reforms in sectors affected by the changes. The innovation in e-Health creates an urge for health sectors to define structure and organizational changes. Attempts that are made to reform Middle East’s health sector have been met with notable problems that, in turn, lead to the slow adoption of technology. Al-Samarraie et al. [6] supported Alajlani & Clarke [5] with the arguments that Middle East’s go-slow in technology adoption results from stakeholders’ resistance. In a study to review progress in adopting and using telemedicine in Middle Eastern countries, Al-Samarraie et al. [6] conducted a literature review on 43 peer-reviewed articles published between 2010 and 2020. The research answered two questions “What is the current progress of adoption and use of telemedicine in the Middle East?” and “What are the key barriers to implementing telemedicine in the two countries?” Al-Samarraie et al. stated there are major cultural barriers affecting e-Health adoption in Middle Eastern countries include religious, traditional beliefs, literacy level, and linguistic barriers. The study also noted that the absence of laws and regulations to support the transformation process affected the sustainable adoption of e-Health. The legal and regulatory framework designed to guide the delivery of care in Syria shows that e-Health may compromise patients’ privacy, which eludes the nursing code of ethics. In addition to the reform challenges, other factors compromising the sustainable adoption of e-Health include organizational (poor training, media representation, insurance, and strategic planning), individual barriers, and poorly motivated healthcare workers.
Al-Samarraie et al, calculated the contribution of different factors in reduced rates of e-Health adoption in Syria as a percentage of the total number of barriers identified from the 43 peer-reviewed articles. The results showed that technological and organizational barriers are the most affecting factors.
Ay et al. [7] expanded on the factors affecting the sustainable adoption of e-Health by conducting cross-sectional, analytical, and observational studies. The study employed snowball sampling and structured questionnaires to collect data from the target population. A total of 196 surveys were carried out by a non-government organization in Jordan hosting Syrian refugees. Ay et al. findings align with both Alajlani & Clarke [5] and Al-Samarraie et al. [6] in that structural and social barriers limited the implementation of e-Health among Syrian refugees. The study’s findings provided insights to humanitarian organizations wishing to support Syria and other developing countries to adopt e-Health.
International intervention can facilitate the adoption of e-Health in Syrian. However, the government should evaluate its current situation to determine if the factors within its jurisdiction hinder the successful implementation of e-Health interventions. Granja, et al. [8] carried out a systematic review to evaluate the factors influencing the outcomes of e-Health intervention. The study found that e-Health intervention’s success depends on its perceived impacts on healthcare. According to Granja, et al [8], research on e-Health should be carried out before implementing the desired intervention. Even though Granja, et al did not directly contribute to Syria’s case study, they informed the research topic from the perspective of Syria’s current situation. Alajlani & Clarke [5] found that healthcare practitioners in Syria have the required awareness to support e-Health. The latter findings align with Granja, et al [8] whose finding indicates that research is a critical factor in defining the success of e-Health intervention. The fact that healthcare practitioners in Syria are not conversant with e-Health technology implies that they cannot explore e-Health. The overall impact is the unsustainable adoption of e-Health. The study also noted that the ICT barrier also challenges the sustainable implementation of e-Health in Syria.
Information Technology Barriers
Information and communication technology have been perceived as enablers of economic development. A notable discrepancy is, however, noted in developing countries whereby the poor are, in most cases, left out of enjoying the benefits of ICT. Touray, et al. [9] conducted a study to identify ICT barriers in literature and empirical findings and categorize the barriers into critical success factors. The study employed a systematic literature review and case study methodologies. The review analyzed 1107 articles published between 2000 and 2011, while the empirical data was collected through a total of 200 questionnaires to evaluate internet adoption at user levels. The achieved data were analyzed using open coding and non-hierarchical coding. The study found 43 ICT barriers using two different studies. Forty of the identified barriers were common in the two studies, while three arose from the empirical study findings. According to Touray, et al. [9], economic socio-culture (SC), economical (EC), infrastructure (IF), legal and regulatory (LR), technical (TN), and education skills (ED) compromised the adoption of e-Health in developing countries. The study concluded that politics and leadership and lack of internet exchange points are major barriers affecting e-Health adoption in developing countries.
Even though the study was not conducted in Middle Eastern countries, its findings align with the reports previously evaluated in this study. The three outstanding barriers affecting the adoption of e-Health in developing countries include lack of internet exchange points, interference from foreign governments, and micromanagement of e-Health.
Civil Conflicts
Regions with political instability and wars suffer numerous economic challenges that increase government spending on vital activities. Irrespective of the benefits of e-Health, the Syrian government has more stressed economic issues to handle from the ongoing war. In a study to evaluate the impacts of the Syrian war on the implementation of e-Health, Bowsher et al. [10] employed narrative hermeneutic methodology. The literature review included articles composed from 2000 onwards, whereas thematic analysis deduced common themes. According to Bowsher et al., altered security conditions in Syria require the healthcare sector to adopt and revise partial online training programs instead of focusing on in-person care delivery. The latter requirement does not align with the e-Health framework because e-Health offers in-person healthcare services. The role of e-Health in regions with political and civil instability is to expand and facilitate the delivery of care. It is, however, challenging that many regions with civil disruptions do not have the right resources to support the implementation of e-Health. Even though Bowsher et al. [10] have provided a detailed explanation of the effects of war on e-Health, their findings differ from previous findings [5-7]. The latter studies connected the poor adoption of e-Health in Syria to cultural, organizational, and social barriers. Bowsher et al. [10] explained the go-slow in e-Health adoption with arguments that conflicts require frequent changes in healthcare provision strategies, a move that requires plenty of resources. The scarcity of resources in Syria and many other developing nations makes it hard for the healthcare sector to adopt e-Health. However, Bowsher et al. agreed with previous studies that a lack of professional training also compromises the adoption of e-Health in Syria.
Factors affecting clinician adoption of mobile health tools
Clinician’s attitude towards a healthcare innovation plays a critical role in defining the success or failure of the healthcare innovation. Jacob, et al. [11] article reported the findings of a structured review article to explore the relevance of published studies regarding social, organizational, and technological factors compromising the adoption of e-Health in developing countries. The study evaluated 171 peer-reviewed articles from MEDLINE, PubMed, SAGE, and Cochrane online databases. Technological factors defining clinicians’ adoption of e-health include outdated systems, system errors, poor quality outcomes, and data security issues [11]. Even though technological barriers are crucial in hindering the sustainable adoption of e-Health, workflow-related factors arose as the main factor from the contacted literature. The world is witnessing a notable shortage of healthcare workers. This implies that nurses and other health care practitioners have tight fixtures to attend to, which leaves them no time to invest in advancing their technological skills. The situation in developing countries is worse because, apart from the shortage of healthcare providers, the region does not have enough resources to invest in continuous nurses training programs. Even though Jacob et al. concentrated on identifying physician-related factors, their findings relate to most of the articles contacted earlier in this review. For instance, technological factors identified in [5,8,9] are also highlighted in Jacob, et al study [11].
Decrease in physician-to-patient ratio
According to World Bank Report (2015) [12], the physician-to-patient ratio has been decreasing tremendously since the onset of the Syrian war. For instance, Syria’s physician-to-patient ratio has been declining since the onset of the war, from 1:370 to a current ratio of 1:546. Stephan [13] supported the latter ideology with findings that 30% to 60% of Syrian physicians have left their country.
Challenges in the adoption processes of e-Health
Zayyad & Toycan [14] highlighted how adopting e-Health technology in developing countries is crucial in managing healthcare facilities while ensuring they offer quality services to patients. They used a modified technology acceptance model (TAM) to highlight how to facilitate the implementation of electronic health records (EHR), and the reasons why the process should be undertaken in phases. However, as the facilitator, the Syrian government should bring the reality check to the table and display why the new EHR system benefits the health sector and healthcare dispensation. In this context, the impediment factors from different stakeholders in the sector should be handled at the initial stages to ensure a smooth transition. In essence, the most important factor that should be considered is how the communication, practicability, and implementation of the EHR system are supposed to be embraced by all the stakeholders involved because they will be vital in running the technological system.
Using the narrative hermeneutic methodology, Alajlani & Clarke [5] found five qualities that should be handled before the diffusion of innovation and invention of new technologies in any healthcare setting, and these adaptations help to ensure the success of the procedure. Individual attitudes also play a critical role in this process of adopting new technologies, and due to that reason, people are concerned with five qualities. These include relative advantage: where the individuals adopting the new innovation must see how it will improve the old ways of doing things. In addressing this issue, Syrian healthcare professionals are supposed to be taken through the way that the accessibility and the availability of patient information under the new system will reduce the time unless when they were using the old system. The latter findings were supported by Said [15], who used Egypt’s healthcare to highlight how under EHR, the patient’s past and current medical information are accessible with a single click and input of the relevant data. This will ensure that they can be assisted faster during an emergency because different healthcare professionals can view their medical history under one platform.
Learning Measures for Improving e-Health
Matlin et al. [16] used qualitative research methods to highlight the Syrian government’s role in the EHR system implementation to improve healthcare safety, efficiency, and quality, especially during the refugee crisis. Furthermore, the government is supposed to guarantee that it protects the patient’s privacy and personal rights as it is envisioned under the law. Namatovu & Semwanga [17], supported the latter study’s finding with qualitative research to learn how the process of presenting the EHR system compromises its adoption in Syria. The reason for their involvement is that they will be responsible for training the individuals who will take part in the final phase of inputting the patient’s information into the new system. Syria is a religious and conservative country that follows Islamic laws and principles, and it is vital to use these approaches to ensure civic education is available for all the people involved. Therefore, the transition from the traditional form of handling patient information is supposed to be put into the new system, and it should be carried out with utmost responsibility and care to avoid errors and misuse of the new data.
Shawahna [18] used CDSS systems research to indicate how the efficacy and quality delivery of Syrian and other Middle East countries healthcare in both rural and urban areas rely on communication, interaction, and association with various care providers, medical residents, physicians, nurses, and other interested parties in the medical field. Therefore, when the different stakeholders converge for the meeting, they should be made to understand that the change in the EHR system does not only impact them; it is a collective responsibility of all the other parties with whom they interact daily. The transition to electronic health records (EHR) is not an easy task for any health center or for the physicians, the hospital management, the members of staff, and the nurses who are usually at the center of these changes because they make the transition to become easier [17]. The essence of converging healthcare providers and other stakeholders is to ensure that they can understand the importance and significance of having operational electronic health records (EHR) and how it will change their lives.
In the initial process of implementing electronic health records (EHR), all interested parties should be called to stakeholder meetings to be enlightened and educated on their role in the procedure. The meetings should be frequently held during the initial stages to ensure that all parties comply with all the issues they are taught, and they should continue until everyone is conversant with what the EHR entails. The type of information nurses should start with the basic process of how the EHR system works from an outsider’s perspective, the security measures that are put in place to avoid third-party interferences, and the implications that should occur when the nurses breach those terms and conditions [19]. The legal procedures entailed in the EHR system are made in such a manner that they are supposed to be agreed upon by all parties through consent because of the private and personal information they hold. In this context, it means that before the whole EHR process is started, in-house communication, coordination, and planning are supposed to be laid out before implementation.
Significance of e-Health compatibility
Zayyad and Toycan [14] indicate how electronic health and technology should be compatible with the new system while advancing values and practices that ensure the innovation aligns with the healthcare practices of the state or government. In this context, healthcare professionals are supposed to know that the inclusion of technology in how healthcare services are undertaken is a concept meant to infuse the old methods into a new platform. The old information will only be input into the EHR, and no other changes will be initiated because the data in the old system will just be keyed in for easy accessibility. Namatovu & Semwanga [17] supported the earlier applications of e-Health by noting that the simplicity factor should also be part of the new EHR system so healthcare professionals can easily operate the new technology. Based on these analogies, they highlighted how adopters must believe they can easily master the new technology; because if they consider it difficult, the greater the resistance. Therefore, it is the duty of the management and the trainers to use the simplest way possible to ensure that all involved personnel will master the system within a specified time span.
Hossain et al. [20] conducted a study in rural Bangladesh using the TAM model to learn how the trial-ability of the new EHR system should be made before the whole process is fully implemented. The report of Salminen & Mursu [9] also supports this approach, where the trial period should show that all the parties involved in operating EHR can “play around’ with the new technology while exploring its capabilities. The trial period of any new technology comes with the chance for the adopters to make mistakes so that they can be rectified and changed to a simpler version, if any, is available. Hossain, et al [20] used 292 respondents where through the trials; the seriousness of resisting change by the adopters indicated that new technology could be learned with an open mind. Observable results: the adopter should have adequate evidence, information, and data on how the new EHR has succeeded in other situations. Most of the data and information should highlight EHR’s success, especially in bigger health centers that have included technology in all their services and their rate of offering quality services to their patients. Therefore, when the smaller healthcare centers adapt to the new changes, it is only meant to ensure that they are not left out when the whole system changes, and they familiarize themselves with technology in all their healthcare delivery [10]. In all these adaptations, it will help the nurses to have an open mind that when they advance in their careers, the bigger health centers are also using the technology, and therefore, it is essential for them to learn on a low-level scale before they are enrolled in other complex EHR systems.
Summary findings:
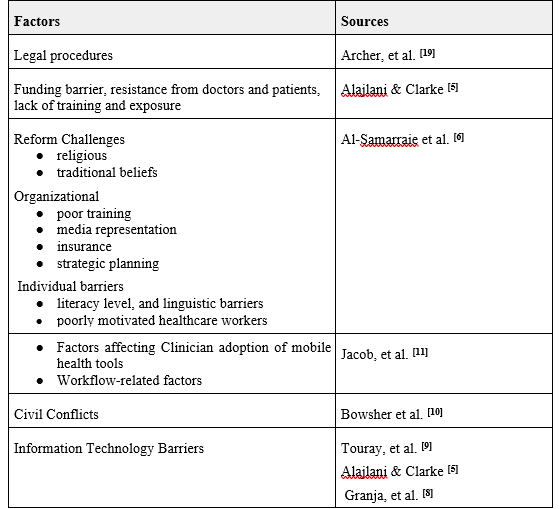
By providing a clear and concise summary of the key findings from the literature, Table 1 could help to inform decision-making, guide the development of interventions and policies, and identify areas for future research.
Table 1. A summary findings table listing the barriers of implementing e-Health in developing countries based on research papers.
CONCLUSION
Electronic health is among the most promising trends in healthcare. Implementing e-Health is associated with many benefits to the healthcare department and other stakeholders in the healthcare docket. Irrespective of the benefits of e-Health, developing countries are lagging behind in its adoption. Using a case study of Syria, this article has identified some major challenges compromising the sustainable adoption of e-Health in developing countries. The most conspicuous challenge affecting arose from the lack of training and exposure to e-Health affected Syrian health professionals more than in Jordan [5]. Additionally, cultural barriers (religious, traditional beliefs, literacy level, and linguistic barriers) also compromised the sustainable adoption of e-Health [9]. The ongoing war in Syria negatively affected the implementation of e-Health since the government does not have adequate resources to facilitate the implementation process. Altered security conditions in Syria require the healthcare sector to adopt and revise partial online training programs instead of focusing on in-person care delivery. The latter requirement does not align with the e-Health framework because e-Health offers in-person healthcare services. In summary, the unsustainable adoption of e-Health in Syrian and other developing countries can be classified into three categories that, include social, systematic, economic, and organizational barriers.
RECOMMENDATION
Improving e-Health adoption in Syria and other developing countries is indeed crucial for advancing healthcare services and ensuring better access to medical facilities. Implementing effective measures to increase the consumption of e-Health requires a multi-faceted approach. We here list several proposed strategies:
Continuous Training for Healthcare Practitioners
Subjecting healthcare practitioners to continuous training on emerging technologies is an excellent step. It will equip them with the necessary skills and knowledge to effectively use e-Health tools and technologies in their practice. This approach helps address the issue of brain drain, where physicians leave the country in search of better opportunities abroad. By offering up-to-date training, the country can retain skilled professionals and attract others who want to work in a technologically advanced healthcare environment.
Investing in Modern Technology
Investing in modern technology is essential for upgrading healthcare facilities and providing healthcare practitioners with the tools they need to adopt e-Health practices. This could include providing hospitals and clinics with the necessary infrastructure, such as electronic health record systems, telemedicine platforms, and remote monitoring devices. By making these technologies available, healthcare practitioners can become more familiar with and embrace e-Health solutions.
Learning from Jordan’s Experience
Drawing insights from Jordan’s experience can be beneficial. As Jordan introduced e-Health technology earlier, it can serve as a valuable case study for Syria to understand the benefits, challenges, and best practices in implementing e-Health initiatives. This information can guide Syria in making informed decisions and avoiding potential pitfalls in its e-Health adoption process.
Addressing Cultural and Systemic Barriers
Cultural and systemic barriers can impede the successful adoption of e-Health in Syria. To overcome these challenges, investing in community-based education programs is essential. These programs should focus on educating healthcare practitioners and community members about the advantages of e-Health and dispelling any misconceptions or fears related to its implementation. By involving the community in the process, acceptance and support for e-Health initiatives can be significantly improved.
Encouraging E-Health Research
With a growing adoption of e-Health practices, there is an opportunity for Syria to invest in e-Health research. Research in this field can help identify areas for improvement, measure the impact of e-Health technologies on patient outcomes and healthcare costs, and refine the implementation strategies for better results.
Collaboration with International Partners
Syria can also benefit from collaborating with international partners and organizations experienced in e-Health adoption. These collaborations can provide technical expertise, financial support, and access to best practices, helping Syria leapfrog some challenges and accelerate its e-Health transformation.
In summary, enhancing e-Health adoption in Syria requires a comprehensive approach that includes continuous training for healthcare practitioners, investment in modern technology, learning from other countries’ experiences, addressing cultural and systemic barriers through community-based education, encouraging research, and fostering international collaboration. By implementing these strategies, Syria can pave the way for more efficient and effective healthcare delivery through e-Health solutions.
References :- Elharish F, Denna S, Maatuk IM, Elberkawi E. Application of electronic health records in polyclinics: barriers & benefits. In International Conference on Data Science, E-learning and Information Systems 2021 (pp. 40-46). Available from: https://doi.org/10.1145/3460620.3460628 Subscription required.
- Allahham L, Mouselli S, and Jakovljevic M. The quality of Syrian healthcare services during COVID-19: a HEALTHQUAL approach. Frontiers in Public Health, 10, 970922, 2022. Available from: https://doi.org/10.3389/fpubh.2022.970922 .
- Karasapan O. The war on Syria’s health system. 2016, Available from: https://www.brookings.edu/blog/future-development/2016/02/23/the-war-on-syrias-healthsystem/#:~:text=According%20to%20a%20report%20by,with%20more%20on%20the%20way .
- Pishnyak A., and Khalina N. Perception of new technologies: constructing an innovation openness index. Форсайт, 15(1 (eng)) 2021, 39-54. Available from: http://dx.doi.org/10.17323/2500-2597.2021.1.39.54 .
- Alajlani M, and Clarke M. Effect of culture on acceptance of telemedicine in Middle Eastern countries: a case study of Jordan and Syria. Telemedicine and e-Health, 2013, 19(4), 305-311. Available from: https://doi.org/10.1089/tmj.2012.0106 Subscription required.
- Al-Samarraie H, Ghazal S, Alzahrani AI, and Moody L. Telemedicine in Middle Eastern countries: Progress, barriers, and policy recommendations. International journal of medical informatics, (2020) 141, 104232. Available from: https://doi.org/10.1016/j.ijmedinf.2020.104232 Subscription required.
- Ay M, Arcos González P, and Castro Delgado R. The perceived barriers of access to health care among a group of non-camp Syrian refugees in Jordan. International Journal of Health Services, (2016), 46(3), 566-589. Available from: https://doi.org/10.1177/0020731416636831 Subscription required.
- Granja C, Janssen W, and Johansen MA. Factors determining the success and failure of e-Health interventions: systematic review of the literature. Journal of medical Internet research, (2018), 20(5), e10235. Available from: https://doi.org/10.2196/10235 .
- Touray A, Salminen A, and Mursu A. ICT barriers and critical success factors in developing countries. The Electronic Journal of Information Systems in Developing Countries, (2013), 56(1), 1-17. Available from: https://doi.org/10.1002/j.1681-4835.2013.tb00401.x .
- Bowsher G, El Achi N, Augustin K, et al. e-Health for service delivery in conflict: a narrative review of the application of e-Health technologies in contemporary conflict settings. Health policy and planning, (2021), 36(6), 974–981. Available from: https://doi.org/10.1093/heapol/czab042 .
- Jacob C, Sanchez-Vazquez A, and Ivory C. Social, Organizational, and Technological Factors Impacting Clinicians’ Adoption of Mobile Health Tools: Systematic Literature Review. JMIR mHealth and uHealth, (2020), 8(2), e15935. Available from: https://doi.org/10.2196/15935
- Zayyad MA, and Toycan M. Factors affecting sustainable adoption of e-Health technology in developing countries: an exploratory survey of Nigerian hospitals from the perspective of healthcare professionals. PeerJ, (2018) 6, e4436. Available from: https://peerj.com/articles/4436/
- Said GRE. Factors Affecting mHealth Technology Adoption in Developing Countries: The Case of Egypt. Computers, (2022), 12(1), 9. Available from: https://www.mdpi.com/2073-431X/12/1/9
- Matlin SA, Depoux A, Schütte S, et al. Migrants’ and refugees’health: towards an agenda of solutions. Public Health Reviews, (2018), 39(1), 1-55. Available from: https://publichealthreviews.biomedcentral.com/articles/10.1186/s40985-018-0104-9
- Namatovu HK, and Semwanga AR. Barriers and Facilitators of e-Health Adoption among Patients in Uganda–A Quantitative. (2021) Available from: https://www.preprints.org/manuscript/202108.0487/v1
- Shawahna R.. Merits, features, and desiderata to be considered when developing electronic health records with embedded clinical decision support systems in Palestinian hospitals: a consensus study. BMC medical informatics and decision making, (2019), 19(1), 1-21. Available from: https://bmcmedinformdecismak.biomedcentral.com /articles/10.1186/s12911-019-0928-3
- Archer N, Lokker C, Ghasemaghaei M, and DiLiberto D. e-Health implementation issues in low-resource countries: model, survey, and analysis of user experience. Journal of Medical Internet Research, (2021), 23(6), e23715. Available from: https://www.jmir.org/2021/6/e23715/
- Hossain N, Yokota F, Sultana N, and Ahmed A. Factors influencing rural end-users’ acceptance of e-Health in developing countries: a study on portable health clinic in Bangladesh. Telemedicine and e-Health, (2019), 25(3), 221-229. Available from: https://www.liebertpub.com/doi/10.1089/tmj.2018.0039 .
- World Bank (2015). Syria SY: Physicians: per 1000 People. Available from: https://www.ceicdata.com/en/syria/health-statistics/sy-physicians-per-1000-people .
- Stephan L. Syria Faces Shortage of Doctors. (2022) Available from: https://www.lemonde.fr/en/international/article/2022/06/11/syria-faces-shortage-of-doctors_5986469_4.html.
Fund: No funding is allocated for this work.
Author contributions:
Supervision: Bassel AlKhatib
Writing – original draft: Mouhamad Kawas.
Writing – review & editing: Bassel AlKhatib
Data and materials availability: All data are available in the main text.
Competing Interests :The Authors declare that they have no competing interests.
(ISSN - Online)
2959-8591
