For quite some time now, the world has been witnessing a radical shift towards the virtual world in various fields, where financial and commercial transactions and many other fields are now carried out entirely through electronic applications, even official and government transactions, most of which are also took place via Internet. The recent circumstances that the world has witnessed (Corona, wars…) have greatly demonstrated the importance of virtual reality, especially artificial intelligence and deep learning, as these circumstances imposed the importance of many human activities not being linked to the real presence of people. One of the most important activities affected by this new trend is commercial activities, as the localization of e-commerce technology has become of great importance and necessity. On the other hand, the new information fields of artificial intelligence and deep learning provide many advanced tools to localize this technology. There is no doubt that the development in the field of digital transformation has made great strides in many fields, and many activities have now been carried out entirely over Internet using appropriate applications. It is natural that the expansion of digital transformation’s control over commercial activity is related to the development of tools and algorithms that enable us creating applications suitable for each field. Another important justification for this study is the lack of programs that support remote shopping in an interactive way that simulates the process of traditional presence in the store. Based on a review of previous studies in the field of virtual clothing [1], it has become clear that most of the proposed models have limitations related to the data on the target clothing and the people wearing those clothing. In this review, we conduct a comparative study on investing deep learning and deep fake algorithms to choose the best three-dimensional digital models of colored clothing and reveal their attributes [2][3][4]. This topic needs to address several axes, the most important of which are studying the digital models used in deep learning algorithms, studying algorithms for human body detection and determining reference points that correspond to digital models [5][6], and studying deep fake algorithms to give a real impression about clothing these models [7].
GENERAL METHODOLOGY
According to studies, virtual fitting rooms adopt AI techniques, deep learning algorithms, and neural networks to develop virtual try-on clothes. One of the most widely used learning algorithms is convolutional neural networks (CNN) (Figure 1), which is used to prepare 3D networks of the human body and can be generalized to different body shapes and poses.
Figure 1: An example of the main layers of a CNN
The general architecture of generative models based on CNN consists of:
Dataset including multiple meshes of clothed human scans, different types of outfits, and different poses.
Encoder
Decoder
Discriminator
CNN is compatible with the famous Skinned Multi-Person Linear Model (SMPL) body model, which is defined as a realistic 3D model of the human body based on extracting and blending shapes through thousands of 3D body scans [8]. SMPL is more accurate than other models and is compatible with existing graphic pipelines. It is viewed as skinned vertex-based model that accurately represents a wide variety of body shapes in natural human poses. One of the latest network models is the Clothed Auto Person Encoding (CAPE) that provides SMPL mesh-registered 4D scans of people wearing cloths, along with recorded scans of real body shapes under clothing [9]. CAPE adds two stages to the general architecture as follows (Figure 2):
Figure 2: CAPE network architecture [9]
Condition module: For pose θ, CAPE removes non-clothing parameters, e.g. head, hands, fingers, feet and toes, resulting in 14 valid joints from the body. The pose parameters from each joint are represented by the flattened rotational matrix. This results in the overall pose parameter R, which feeds into a small fully-connected network θ. The clothing type C refers to the type of “outfit”, i.e. a combination of upper body clothing and lower body clothing. As the types of clothing are discrete by nature, CAPE represents them using a one-hot vector, C, and feeds it into a linear layer.
Conditional residual block (CResBlock): CAPE adopts the residual block (ResBlock) from Kolotouros et al. [11] which includes ensemble normalization [13], nonlinearity, a graph convolutional layer and a graph linear layer. After input to the residual block, CAPE appends a state vector to each input node along the feature channel. ResBlock is the graph residual block from outputs on each node.
RELATED WORK
The related works can be classified into three axes:
Reconstructing 3D humans:
Reconstruction of 3D human’ bodies from 2D images and videos is a classical computer vision problem. Most approaches [18, 32] output 3D body meshes from images, but not clothing. This ignores image evidence that may be useful. To reconstruct clothed bodies, methods use volumetric [20, 30] or bi-planar depth representations [12] to model the body and garments as a whole. While these methods deal with arbitrary clothing topology and preserve a high level of details, the reconstructed clothed body is not parametric, which means that the pose, shape, and clothing of the reconstruction cannot be controlled or animated. Another group of methods is based on SMPL [25, 31]. They represent clothing as an offset layer from the underlying body as proposed in Cloth Cap [28] as shown in (Figure 3). These methods can change the pose and shape of the reconstruction using the deformation model of SMPL. This assumes that clothing deforms like an undressed human body; i.e. clothing shape and wrinkles do not change as a function of pose.
Figure 3: ClothCap approach [28]
Parametric models for 3D bodies and clothes
Statistical 3D human body models learned from 3D body scans [23, 32] capture body shape and pose and they are an important building block for multiple applications. Most of the time, people are dressed and these models do not represent clothing. In addition, clothes deform as we move, producing changing wrinkles at multiple spatial scales. While clothing models learned from real data exist, few can be generalized to new poses. For example, Neophytou and Hilton [34] proposed to learn a layered garment model from dynamic sequences, but generalization to novel poses is not demonstrated. Yang et al. [27] trained a neural network to regress a PCA-based representation of clothing, but they proved the generalization on the same sequence or on the same subject. Lahner et al. [29] proposed to learn a garment-specific pose-deformation model by regressing low-frequency Principal Components Analysis (PCA) components and high frequency normal maps. While the visual quality was good, the model is garment-specific and does not provide a solution for full-body clothing. Similarly, Alldieck et al. [25] as shown in (Figure 4) used displacement maps with a UV parametrization to represent surface geometry, but the result was only static. Wang et al. [24] allowed manipulation of clothing with sketches in a static pose. The Adam model proposed in [23] can be considered clothed but the shape is very smooth and not pose-dependent. Clothing models have been learned from physics simulation of clothing [19, 33], but the visual reliability was limited by the quality of the simulations.
Figure 4: Displacement maps with a UV parametrization to represent surface geometry [25]Generative models on 3D meshes
CAPE model predicts clothing displacements on the graph defined by the SMPL mesh using graph convolutions [10]. However, there is an extensive recent literature on methods and applications of graph convolutions such as [21, 26]. Most relevant here, Ranjan et al. [26] proposed to learn a convolutional auto encoder using graph convolutions with mesh down- and up-sampling layers [13]. Although it worked well for faces, the mesh sampling layer made it difficult to capture the local details, which are key in clothing, while CAPE captures local details by extending the PatchGAN [22] architecture to 3D meshes (Figure 2).
COMPARISON AND DISCUSSION
Comparing between public 3D clothed human datasets according to six points (Captured, Available Body Shape, Registered, Large Pose Variation, Motion Sequence, High Quality Geometry) leads to the following results:
Inria Dataset presented an approach to automatically estimate the human body shape under motion based on a 3D input sequence showing a dressed person in possibly loose clothing.
It has no registered 3D meshes of clothed human scans. It has limited variation in pose and low quality geometry [14] (Figure 5).
BUFF Dataset introduced a method to estimate a detailed body shape under clothing from a sequence of 3D scans. This method exploits the information in a sequence by merging all clothed registrations into a single frame as shown in (Figure 6).
BUFF Dataset is like Inria but has high quality geometry [15].
Figure 5: Inria Dataset approach [14]Figure 6: Qualitative pose estimation results on BUFF dataset [15] Left to right: scan, Yang et al. [27], BUFF result
Adobe Dataset key insight is to use skeletal pose estimation for gross deformation followed by iterative non-rigid shape matching to fit the image data.
Adobe Dataset does not have human body shapes. It has limited variation in pose and low quality geometry [12]. 3D people dataset proposed a new algorithm to perform spherical parameterizations of elongated body parts, and introduced an end-to-end network to estimate human body and clothing shape from single images, without relying on parametric models, (Figure 7).
3D People Dataset contains all the points but lacks the ability to capture and convert data from different sources [10].
Figure 7: Annotations of the 3D People Dataset [10]
CAPE Dataset contains all the points, as shown in (Figure 8). Given a SMPL body shape and pose (a), CAPE adds clothing by randomly sampling from a learned model (b, c), and can generate different clothing types — shorts in (b, c) vs. long-pants in (d). The generated clothed humans can generalize to diverse body shapes (e) and body poses (f).
Figure 8: CAPE model for clothed humans [9]
Characterized by accurate alignment, consistent mesh topology, ground truth body shape scans, and a large variation of poses, CAPE features make it suitable not only for studies on human body and clothing, but also for the evaluation of various Graph CNNs. However, CAPE differs from the other methods in learning a parametric model of how clothing deforms with pose. Furthermore, all the methods of Parametric models are regressors that produce single point estimates. In contrast, CAPE is generative, which allows to sample clothing. A conceptually different approach infers the parameters of a physical clothing model from 3D scan sequences was proposed in [17]. This can be generalized to novel poses, but the inference problem is difficult and, unlike CAPE, the resulting physics simulator is not differentiable with respect to the parameters. Since the presented results confirmed the investment of deep fake in the field of virtual dressing, we are on the way towards investing in artificial intelligence and neural networks in this field, in parallel with the very rapid development in electronic clothing marketing, and in response to the requirements of the local and global market in this field.
CONCLUSION
Although the results of the previous studies are significant, the research remains open due to the limitations of the approved methods, which can be summarized as follows:
The limitation of the offset representation for clothing such as skirts and open jackets differ from the body topology and cannot be represented by offsets as shown in (Figure 9). Mittens and shoes can technically be modelled by the offsets, but their geometry is sufficiently different from that of fingers and toes, making this impractical.
Dynamics issues: the approved models take a long time to train the algorithms, because the generated clothing depends on pose, and does not depend on dynamics. This does not cause a severe problem for most slow motions but cannot be generalized to faster motions.
Future work will address models of clothing, but instead of scanning the entire body, we propose to consider sufficient features on the body to estimate the shape of the body which may be sufficient for virtual dressing. Therefore, one will not need to photograph the body completely naked or with a minimum amount of clothing, as we propose to conduct an investigation of certain points of the body. Another restriction can be added to make the work easier is to deal with the human body as two parts, upper and lower, based on the International Standard Organization (ISO) standards to assign points to the human body [16].
Figure 9: Qualitative results on fashion images [9] SMPL [8] results are shown in green, CAPE results are in blue
Phytoplasmas, classified as wall-less and uncultivable bacteria, comprise a group of prokaryotic plant pathogens that inhabit the phloem of plant hosts as well as the salivary glands of the insects that act as their vectors [1, 2]. They were first identified when in 1967, Doi and co-workers discovered pleomorphic bodies in infected samples from mulberry trees and other plants that were infected by yellows diseases [3]. Previously, it had been believed that most yellowing diseases were caused by viruses because they were generally transmitted by insects, but many yellows-type diseases are now known to be caused by phytoplasmas [4]. The initial name of phytoplasmas was mycoplasma-like organisms (MLOs) due to ultrastructural and morphological similarities to mycoplasmas and because the mycoplasmas that cause diseases in humans and animals have similar sensitivity to tetracyclines. The name (MLOs) was used for phytoplasmas until 1994 [3] when the International Committee on Systematic Bacteriology (ICSB) sub-committee on the taxonomy of Mollicutes agreed to rename them as ‘Phytoplasmas’ to discriminate against them from other bacteria which belong to the class Mollicutes. Phytoplasmas were given this new name because of specific characteristics, such as their phytopathogenic properties, which do not exist in either mycoplasmas or other MLOs that inhabit phloem sieve tubes [5].
Morphology and genomic characteristics
The morphology of phytoplasmas is different from other bacteria and they have a range of sizes from 200 to 800nm and appear under an electron microscope as filamentous and pleiomorphic bodies [6] (Fig. 1). It has been suggested that there are filamentous forms of phytoplasmas and the reason for the phytoplasma size differences is that these represent different developmental stages in their plant hosts. In addition, their cell walls lack a rigid cell wall and have just a single unit cell membrane [6]. The genomes of Phytoplasmas are among the smallest in bacteria, between 530 kb and 1350 kb; the tomato strain of the stolbur phytoplasma and a Bermuda grass white leaf phytoplasma represent the largest and smallest genomes known [7]. Generally, the main reason for the limited studies of phytoplasma diseases has been the lack of ability to culture them in vitro, which may be related to their lack of essential genes, such as genes for biosynthesis of nucleotides, fatty acids, and amino acids [1, 9]. In addition, while most bacteria have a phosphotransferase system, which is important for phosphorylation and import of sugars (sucrose, fructose, and glucose), phytoplasmas do not have this system which makes them highly dependent on their plant hosts to get nutrients [10].
Figure 1 Electron microscopy picture (6000x) of a cross-section of sieve tubes with phytoplasmas, modified from [8].
Pathogenicity of phytoplasmas
The study of phytoplasmas has been difficult because no reliable phytoplasma culturing has been accomplished in vitro, so that understanding of phytoplasma pathogenicity is limited. The majority of gene expression results and genome studies in vitro have been based on creating transgenic plants expressing phytoplasma genes in Nicotiana benthamiana or Arabidopsis thaliana. Evidence suggests two main factors affect phytoplasma pathogenicity: virulence factors and protein secretion.
Virulence factors
There are two main factors that appear to give the phytoplasmas their severity; the first factor is that several genes in phytoplasmas encode effector proteins that act directly on the host plant. The second is the side effects of phytoplasma infection [11]. For the first factor, a number of genes have been found in phytoplasmas that act as virulence factors and appear to be responsible for pathogenicity. For example, Bai et al [12] reported that the SAP11 protein, which is one of 56 secreted proteins by AY-WB phytoplasma (SAPs), contains a nuclear localization signal (NLS) and targets the nuclei of host cells, and also contains an N-terminal signal protein (SP). In addition, Sugio et al [13] reported that SAP11 expression increased in the AY-WB insect vector Macrosteles quadrilineatus offspring. For the second factor, and since phytoplasmas lack many important genes such as for metabolite synthesis and metabolic pathways, phytoplasmas must obtain many nutrients from their hosts and the depletion of nutrients from plants causes some of the symptoms of phytoplasma diseases [9]. Furthermore, the OY-W strain of the onion yellows phytoplasma has been shown to possess two glycolytic gene clusters which is a higher copy number than in the OY-M stain. It has been suggested that the harsh symptoms caused by the OY-W strain compared with the mild strain are because of the higher utilization of the carbon source resulting from possessing this increased number of glycolytic genes [9].
Protein secretion
When phytoplasmas are transmitted from diseased plants to healthy plants by insect vectors they enter inside the system of phloem cell cytoplasm [14]. After that, phytoplasmas start multiplying and secreting proteins inside the cytoplasm of phloem cells and some of these proteins are small enough in size to be able to move to other cells of the plant [10]. Phytoplasmas have two main systems to secrete proteins; the first system is called the Sec system for integrating and secreting proteins into cells of plant hosts, and the second one is the YidC system which is integrating membrane proteins [15].For the Sec protein secretion system, this system in Escherichia coli involves three stages; the first is called ‘targeting’, in which a protein is guided by the SecB protein and the signal-recognition particle (SRP) to exit locations in the membrane. The second stage is called ‘translocation’, in which the guided protein uses the action of the SecA, SecE and SecG proteins and nonessential subunits (SecD and SecF) to cross the lipid bilayer. The third stage is called ‘release’, in which the translocated protein is released and allowed to be natively folded in the periplasm or to proceed to the outer membrane for integration. It has been shown from whole genome sequencing of phytoplasmas, including Strawberry lethal yellows (SLY) [16], ‘Candidates Phytoplasma australiense’ strain PAa [17], ‘Candidatus Phytoplasma mali’ strain AT [18], ‘Candidates Phytoplasma asteris’ strain witches’ broom (AY-WB) [19], and ‘Candidates Phytoplasma asteris’ strain OY-M [20], that genes encoding SecA, SecE, and SecY are present in all five genomes. The YidC protein secretion system is also believed to be a common system in phytoplasmas, because the gene encoding the YidC protein has been found in all sequenced phytoplasma genomes [15]. Furthermore, a study conducted by Serek et al [21] revealed that in E. coli, YidC plays a crucial role in ensuring the precise insertion of newly synthesized membrane proteins into membranes. Additionally, it operates independently of the Sec-dependent protein machinery.
Classification of phytoplasmas
As phytoplasmas currently cannot be consistently cultivated in a laboratory setting, their classification remains a challenge. They are classified into the ‘Candidatus (Ca.) Phytoplasma (P.)’ taxon. In this system, if the similarity of the 16S rRNA gene is less than 97.5%, a new ‘Ca. P. species’ can be designated and separated from previously classified ‘Ca. P. species’. Sometimes, if there is a sufficiently different host range and/or insect vectors, a novel ‘Ca. P. species’ can also be created, even if the similarity of the 16S rRNA gene is more than 97.5% [22]. For additional information, and to get a clearer and deeper classification for closely related phytoplasmas, DNA sequences of other genes have been used, such as the spacer between the 16S and 23S rRNA, the ribosomal protein gene (rp), secA, secY and tuf genes [10, 23, 24]. Using the ‘Ca. P. species’ system, phytoplasma have been classified into thirty-three 16S rRNA groups [25-27]. Table 1 (supplementary) provides details of these 16Sr groups, including the name, geographic distribution, and strain/’Ca. P. species’.
Symptoms of phytoplasma diseases
Symptoms in plants can depend on the season, pathogen species, and the stage of disease development, where different organs will exhibit different symptoms. In addition, a few plants can harbor phytoplasmas without showing any symptoms. Symptoms of diseased plants caused by phytoplasma infections include yellowish foliage (discolorations of leaves and shoots) (Fig. 2 and Fig. 3), shoot proliferation (witches’ broom) (Fig. 4), stunting (small leaves and shortened internodes), proliferation (growth of shoots from floral organs) and phyllody (the formation of leaf-like structures in place of flowers) (Fig. 5) [10]. As examples, aster yellows phytoplasma infected plants show witches’ broom symptoms throughout the plant or on flower stalks (Fig. 4), and most of the time only the symptoms on flowers are visible [28]. Elm yellows phytoplasma can cause several different symptoms such as witches’ broom, epinasty, leaf yellowing and decline of Eurasian species (Ulmus spp.) [29]. Napier grass stunt shows clear symptoms of phytoplasma infection on Napier grass plants, such as proliferation of tillers and shortening of internodes, little leaves, leaf yellowing, stunt and eventual death (Fig. 2) [30]. Sometimes the symptoms can be different or very hard to recognize because of complex interference between them and host physiology [31].
Figure 2 Symptoms of Napier grass stunt phytoplasma on Napier grass plants showing leaf yellowing and stunting (Aljafer 2016).Figure 3 Symptoms of Elm yellows phytoplasma on infected Ulmus americana showing yellowing leaves and epinasty compared with a healthy plant on the left side in the picture, modified from [32].Figure 4 Phyllody symptoms on a goldenrod flower infected with aster yellows (Aljafer 2016).Figure 5 Depicts olive trees affected by phytoplasmas, showing shortened internodes, witches’-brooms, and smaller leaves (a), as well as hypertrophied inflorescences (b). This image has been adapted from [32].
Phytoplasma transmission and lifecycle
Transmission of phytoplasmas generally occurs from infected plants to healthy plants through insect vectors feeding on the phloem tissue of diseased plants. Insect vectors can be hoppers (Auchenorrhyncha, Homoptera) or psyllids (Sternorrhyncha, Homoptera) and transmission occurs in a persistent manner. The interactions between phytoplasmas and their insect vectors play a pivotal role in determining the host range of phytoplasmas [4]. Certain insect vectors have the ability to transmit multiple phytoplasma strains, and conversely, specific phytoplasmas can be transmitted by more than one vector. However, the mechanisms of insect vector-phytoplasma specificity or compatibility are not well understood [33].The life cycle of a phytoplasma begins with acquisition feeding, during which the phytoplasma enters the vector through the vector’s stylet while feeding. Subsequently, the phytoplasma traverses the insect’s intestine and is taken up into the hemolymph. Over the course of a few weeks following the initial feeding, it eventually migrates to the salivary gland. During these weeks, phytoplasmas keep multiplying until their concentrations reach a high enough level to be transmitted when the insects start feeding on healthy plants (inoculation feeding) (Fig. 6) [34].
Figure 6 The life cycle of phytoplasmas is depicted with phytoplasmas represented as red dots. It commences with ‘Acquisition Feeding,’ during which an insect, like a leafhopper, acquires phytoplasmas while feeding. Following this, a ‘Latency Period’ ensues, indicating the time it takes for the phytoplasmas to reach an infection titer, necessary for their transmission. The final stage is ‘Infection Feeding,’ during which the insect transmits phytoplasmas to healthy plants as it feeds, modified from [37].
Furthermore, in certain combinations of insect vectors and phytoplasmas, it has been observed that transovarial transmission occurs. This means that the phytoplasma can be passed from parent insect vectors to their offspring. An example of this phenomenon is observed in the case of the leafhopper Matsumuratettix hiroglyphicus and the sugarcane white leaf phytoplasma [35], and the leafhopper Hishimonoides sellatiformis and mulberry dwarf phytoplasma [36]. It is also possible for phytoplasmas to be transmitted by the parasitic plant, dodder (Cuscuta spp.), in experimental conditions. Once dodder plants start growing on infected plants, phytoplasmas enter inside the dodder plant through haustoria and proliferate within the dodder plant, and then move to healthy plants via haustoria of dodder [38]. As an example, European stone fruit yellows, pear decline, and various other phytoplasmas have been intentionally transferred from naturally infected plants to healthy periwinkle plants (Catharanthus roseus) through the use of dodder plants in experimental studies [39]. Přibylová et al [40] reported that dodder plants transmitted RG phytoplasma successfully from infected Rehmannia glutinosa plants to healthy periwinkle plants. In experimental settings, grafting is another method employed for the transmission of phytoplasmas and the maintenance of infected plants. This process involves transferring phytoplasmas from naturally infected plants to healthy ones, often using periwinkle plants as the healthy host. For instance, phytoplasmas have been successfully transmitted from infected grapevines to healthy periwinkle plants through a grafting technique known as wedge grafting [41], and chip and bark grafting has been used to transmit the apple proliferation (AP) phytoplasma from infected apple plants to healthy periwinkle plants [42]. However, grafting has not been successful for all phytoplasmas, and other transmission methods sometimes need to be used. Furthermore, phytoplasmas can also be transmitted through vegetative propagation methods, including storage tubers, cuttings, bulbs, or rhizomes [24].
Phytoplasma diagnostics
The detection of phytoplasmas presents challenges due to their uneven distribution within infected plants and, particularly in woody hosts, their typically low concentration. Historically, researchers attempted various techniques for phytoplasma detection, including grafting onto indicator hosts, electron microscopy observations, and the use of DNA-specific dyes to stain the pathogen’s nucleic acid. However, these approaches often yielded unreliable results. Over the last two decades, the focus in phytoplasma detection has shifted primarily towards serology and, more frequently, nucleic acid-based techniques like PCR (Polymerase Chain Reaction). PCR is employed to amplify specific regions of the phytoplasma genomes that are present within infected plants. Notably, routine diagnostics have evolved from traditional PCR to real-time PCR. This transition has been driven by its enhanced sensitivity and reduced risk of contamination, thanks to the use of a closed system for product detection. Additionally, this method can be adapted for semi-quantitative analysis, further improving its utility in phytoplasma detection and monitoring [43]. Indeed, DNA extraction typically serves as the initial step in diagnosing phytoplasma infections, and many protocols are reported for DNA extraction from potentially infected plants and vectors. Each protocol is different from another and depends on sampling procedures and on the species of plant host/insect or condition of storage in which the collected samples were placed [44-47].
Serological assays
Enzyme-linked immunosorbent assays (ELISA) are one serological method that has been used, but it is rarely used because of the limitations in specificity and sensitivity compared with nucleic acid-based assays. A commercial monoclonal anti-IgG kit-based DAS-ELISA has been developed, but it was unable to detect all ‘Ca. P. mali’ [25].
Nucleic acid-based assays
Polymerase chain reaction
Over the past two decades, the predominant focus in phytoplasma detection research has shifted towards the utilization of nucleic acid-based techniques, particularly Polymerase Chain Reaction (PCR). Researchers have tried to obtain sequences of specific regions of phytoplasma DNA and design primers for these regions. Some of the design involved specific primers for a particular group, but most were trying to design universal or semi universal primers to detect all groups of phytoplasma or most of these groups, of which there are at least thirty-three 16S rRNA groups [4, 27]. Ribosomal RNA primers are one of the sets of universal primers that are generally used to detect phytoplasmas and amplify a specific fragment of phytoplasma DNA (16S rRNA gene). Because of the low concentration of phytoplasma DNA, most laboratories use universal primers in the first round of PCR reactions and then use another internal primer (second round) which is often more specific (nested PCR). There are also ‘universal primers’ for other genes such as the rp (ribosomal operon), secA, tuf, secY, hlg, gyr, and nitroreductase genes [34, 48, 49].Practically, a first round PCR (direct PCR) is performed with a pair of primers, then followed by a second pair of primers which targets primer sites on first round PCR products. Second round PCR assays are created which increase sensitivity and specificity of the diagnosis compared to first round PCR. Figure 7 shows an example of first round and nested PCR primers for the 16S rRNA gene or the spacer region between 16S rRNA and 23S rRNA [50]. From the spacer region (rRNA operon), it is also possible to design specific, semi universal and universal primers. In addition, other genes have been used to obtain high specificity of assays and distinguish between closely related phytoplasma strains, such as ribosomal operon (rp), secA, secY, tuf[34, 51, 52]. Moreover, PCR products can be sequenced and compared against reference phytoplasma sequences on the NCBI database.
Terminal restriction fragment length polymorphism (T-RFLP):
T-RFLP is a technique that has been adapted for the identification of phytoplasmas within their host organisms, including plants and vector insects, as well as for categorizing them into specific phylogenetic groups. In this approach, a fluorescent tag is attached to one of the PCR primers. Subsequently, after performing PCR and enzymatic digestion with a suitable enzyme, the focus is on analyzing the size of the terminal restriction fragment (TRF) that contains the labelled primer. This analysis is typically conducted using automated DNA sequencing equipment [34].
Real-time PCR:
Increasingly, there are new methods to diagnose phytoplasmas, but improvements in diagnostics are needed to produce methods that are more economic, quicker and more robust [53]. Sensitivity of nested PCR protocols is high, but the problem with nested PCR is to obtain high levels of sensitivity without the risk of false positive results due to contamination of samples during the various procedures and opening of tubes [14]. In the last few years, real time PCR (qPCR) which has been used wildly as a tool for phytoplasma diagnosis, replaced standard PCR because of direct reading and high sensitivity of the result. A key characteristics of qPCR is that gel electrophoresis is not needed, which reduces the risk of sample contamination [52, 53].To use qPCR for phytoplasma diagnosis, there are two alternative systems, the first system using SYBR Green [54], and the second uses TaqMan probes [55].The SYBR Green system requires a binding dye for double-stranded DNA, and during qPCR cycles the dye can be detected when it binds double stand qPCR products. The way the SYBR GREEN assay works is as follows. While PCR is happening, PCR products are created because the DNA polymerase amplifies the target sequences. Once the dye is added, it immediately binds to any matched double-stranded DNA and fluoresces. Therefore, every new copy of DNA generated will bind, and as more amplification occurs the fluorescence intensity increases. This can be used as a measure of the amount of product [56].The SYBR-GREEN assay offers several advantages, including its ability to monitor the amplification of any double-stranded DNA sequences without the need for specific probes. This feature helps reducing the overall costs associated with assay setup. However, it comes with a disadvantage: because the SYBR-GREEN dye can bind to any double-stranded DNA, including both target and non-target DNA, there’s a risk of generating false positive signals. Therefore, to ensure accuracy in results, it becomes crucial to carefully design primers that enhance the specificity of SYBR-GREEN assays. Additionally, it’s essential to validate qPCR reactions through melt curve analysis as part of quality control measures [56, 57].
Figure 8 How the SYBR GREEN assay works step by step, modified from [56].
In the TaqMan system and instead of using binding dyes, probes and reporter dyes are used. Probes encode from 5’ to 3’ to target a specific site between a forward qPCR primer site and a reverse qPCR primer site. During cycles of TaqMan reactions, primers start amplifying the DNA target, then probes bind the qPCR products, and the reporter dye is freed from the quencher and detected by the instrumentation of qPCR [58, 59]. In Taqman assays, the probe typically incorporates a fluorescent reporter dye at its 5′ end and a quencher dye at its 3′ end. When the target DNA is introduced, the probe binds downstream from one primer site and becomes susceptible to cleavage by the 5′ end of the Taq DNA polymerase as it extends the primer. During this cleavage step, the reporter dye separates from the quencher dye, resulting in an increased signal emitted by the reporter dye. Once the probe has been cleaved from the target DNA, the primers can continue extending along the template strand until they reach the end. This ensures that the probe does not impede the overall PCR process. During each cycle of PCR, the reporter dye molecules are cleaved from their respective probes, leading to a rise in fluorescence intensity that is directly proportional to the amount of amplicon produced. This fluorescence signal provides a quantitative measure of the target DNA in the sample (see Fig 9) [60].
Figure 9 How Taqman assays work step by step, modified from [61].
TaqMan assays have been developed as universal assays and assays for a number of 16Sr groups (Fig. 9) [14]. In addition, SYBR Green assays have also been developed especially for apple proliferation (AP), bois noir, and flavescence dorée phytoplasmas, and other universal assays to detect phytoplasmas in groups 16SrV, 16SrX, and 16SrXII. When comparing SYBR Green systems to other techniques of phytoplasma detection such as the TaqMan system and conventional nested PCR, the SYBR Green system can give rapid and specific detection of the DNA target of phytoplasmas. For example, assays have been developed to early detection of quarantine phytoplasmas quantitatively, for example ‘Ca. P. pyri’, ‘Ca. P. mali’, and ‘Ca. P. prunorum’ (members of 16SrX group) affecting fruit trees [14].
Loop-Mediated Isothermal Amplification (LAMP):
Recently, the LAMP technique (Loop-Mediated Isothermal Amplification) has been used a lot for phytoplasma detection because it is easy to use and takes a very short time to get the results. This technique amplifes DNA targets under isothermal conditions, and generally uses a set of six primers for each assay (external primers, internal primers, loop primers) and a DNA polymerese with strand displacement activity (Fig. 10). Results of amplifications generally take less than an hour, and can be observed by agarose gel, hydroxyl napthol blue colorimetric assays, or intercalating fluorescent dyes performed in instruments for real-time PCR or LAMP [43, 62, 63]. For example, LAMP assays for two different specific phytoplasma groups have been published; from 16SrI group (aster yellow phytoplasma) and from 16SrXXII group (Cape St. Paul wilt). Sensitivity of these assays was compared to nested PCR, and assays were specific for target DNA phytoplasma [62]. Additional LAMP assays have been developed and documented for the detection of phytoplasma groups 16SrII and 16SrXII in various fruits and weeds found within the Ethiopian Rift Valley. These assays provide valuable tools for identifying and monitoring phytoplasma infections in agricultural and natural ecosystems in this region [43, 63].
How Loop-mediated Isothermal Amplification works:
1. The F2 region (part of FIP primer) hybridizes to region of F2c (part of target DNA) and initiates complementary stand synthesis.2. Similarly, with external primer F3 primer hybridizes to the F3c to the F3c (part of the target DNA) and extends; this leads to the removal of the FIP-linked complementary stand. Those removed stand forms will make a loop at the 5’ end.3. The DNA with a loop at 5’ end becomes a template for BIP, and the same process will happen with B2 and B2c, with hybridization between the B2 region and B2c region of the template DNA.
4. External primer B3 hybridises to B3c (from target DNA) and then extends, leading to removal of the BIP linked complementary stand. These results in the information of dumbbell sharped DNA.
5. DNA polymerase adds nucleotides to the 3’ end to F1, and extends to open the loop at the 5; end. The dumbbell shaped DNA now gets converted to a stem-loop structure and this structure will be useful in the second stage of the LAMP reaction as an initiator for LAMP cycling.
6. During the cycling of Loop-Mediated Isothermal Amplification (LAMP), the Forward Inner Primer (FIP) hybridizes to the stem-loop DNA structure. At this stage, strand synthesis is initiated. Importantly, as the FIP hybridizes to the loop region of the DNA, the original F1 strand is displaced and re-forms as a new loop at the 3′ end of the DNA molecule. This strand displacement activity is a key feature of LAMP and contributes to the exponential amplification of the target DNA.
7. In the next step, the DNA polymerase adds nucleotides to the 3′ end of the B1 region and extends it, which results in the removal of the Forward Inner Primer (FIP) strand. This newly synthesized strand, like before, assumes a dumbbell-shaped DNA structure. Following this, self-primed strand displacement DNA synthesis occurs, leading to the formation of two distinct structures: one complementary to the original stem-loop DNA and another one where any gaps in the structure are repaired, resulting in a stem-loop DNA with no gaps. This process continues as the DNA amplification cycle proceeds in Loop-Mediated Isothermal Amplification (LAMP).
8. After the initial amplification cycle, the two distinct products generated serve as templates for a Backward Inner Primer (BIP) primed strand displacement reaction in the subsequent cycles. This means that with each cycle of LAMP, the target sequence is exponentially amplified. In fact, the amplification rate is so efficient that the target DNA is typically amplified around 13-fold with each half-cycle of LAMP, resulting in a rapid accumulation of DNA copies.
Figure 10 Illustration depicting the operational principle of LAMP assays, involving a set of six primers that consist of external primers (F3 and B3), internal primers (FIP and BIP), and loop primers (loopF and loopB), modified from [64].
The benefits of isothermal amplification techniques include their independence from thermal cycling, simplifying operation, and their lower energy requirements compared to PCR methods, which involve rapid heating and cooling steps. Consequently, it becomes feasible to create compact, battery-powered portable devices. Moreover, in real-time LAMP methods, and similar to real-time PCR, the entire process takes place within sealed tubes, minimizing the potential for sample contamination [65].
Phytoplasma genomics
In the last decade, four phytoplasma genomes have been completely sequenced; ‘Ca. P. asteris’ strains OY-M [20], AY-WB (aster yellows witches’-broom) [19], ‘Ca. P. mali’ strain AT [18] and ‘Ca. P. australiense’ strain PAa [17], and two others have good coverage that is publically available (strawberry lethal yellows SLY) [16], or have been sequenced at the University of Nottingham (Napier grass stunt NGS)[66].
Genome features
According to these genome studies, phytoplasmas SLY, PAa, OY-M, and AY-WB have the larger genome sizes, which are in the order of 960, 880, 853, and 706 kbp. Phytoplasmas AT and NGS have smaller genome sizes of approximately 602 and 484 kbp. Generally, the G+C contents in the phytoplasmas are low; it is from 20.4% to 27.8%. From these six sequenced genomes the NGS has the lowest G+C content which is 20.4%, followed by the AT genome (21.3%), AY-WB genome (26.9%), SLY genome (27.2%), PAa genome (27.4%), and OY-M genome (27.8%). Interestingly, whilst most phytoplasma genomes appear to be circular, that of AT and possibly NGS are linear. The genomes have variable numbers of transfer RNA genes (from 31 to 35), but all of them have two ribosomal RNA operons. Furthermore, four plasmids are found in the genome of AY-WA, two plasmids are found in the genome of OY-M, and one plasmid is found in the genome of PAa and NGS [17-20].
Potential mobile units
Potential mobile units (PMUs) are repetitive genes that are organized in units of approximately 20 kbp, and they are found in many phytoplasma genomes. These PMUs look like composite replicative transposons, and some are associated with putative ‘virulence genes’ and contain several genes for recombination [67]. For example, aster yellows strain AY-WB has four different PMUs including PMU1, PMU2, PMU3, and PMU4. PMU1 is the largest unit at approximately 20 kbp, and the rest of the PMUs have similar gene structures to PMU1, but are smaller. Additionally, PMU1 in AY-WB strain is linear [19, 68]. Up to now, PMUs are regions that have been found and studied in phytoplasma genomes such as ‘Ca. P. asteris’ strain OY-M, ‘Ca. P. australiense’ strains PAa and SLY, and ‘Ca. P. mali’ strain AT. But it is still unclear whether Potential Mobile Units (PMUs) are present in all phytoplasma genomes. The presence of PMUs can vary among different phytoplasma strains and species. While PMUs are commonly found in many phytoplasma genomes and play a role in their genetic diversity and adaptation, the specific distribution of PMUs across all phytoplasma genomes remains an area of ongoing research. Scientists continue to study the genomes of various phytoplasma strains to gain a better understanding of the prevalence and diversity of PMUs in this group of microorganisms [69, 70].
Management and control of phytoplasmas
The primary approach to manage phytoplasmas involves the application of insecticides to regulate the insect vectors responsible for transmission. However, even with the extensive utilization of insecticides, phytoplasma diseases continue to inflict significant damage in numerous countries across the globe [71]. Furthermore, since the usage of chemical control is limited and being reduced worldwide (because of the other effects of chemical materials on humans, plants, animals, and the environment) other approaches are required. In addition, agricultural intensification and climate change are expected to raise insect vector populations, which may lead to more phytoplasma-related yield losses in the future. From current research there is evidence that phytoplasma diseases are becoming widespread worldwide and spreading into new host plants [72].Since antibiotics are too expensive and not a successful or practical strategy for long-time control, using them is not recommended for control of phytoplasmas. In an interesting study from 1985, Dickinson and Townsend, noticed from research on spiroplasmas, which are a group related to plant pathogenic Mollicutes, that remission of symptoms occurred during introduction of specific secondary isolates, with indications that this was because of the presence of lysogenic phages in certain isolates of spiroplasmas. Furthermore, there is evidence that when two different strains of phytoplasmas are mixed together to infect a healthy plant host, some strains can out-compete others. This evidence could be useful for developing the idea of using mild strains as a means of controlling some diseases [73]. Recent experiments at the University of Nottingham have shown that inclusion of two different strains of phytoplasma into healthy periwinkle plants at the same time (RG+SPLL and RG+EY), can result in symptoms that belong to only one 16Sr group (RG) appearing on plants after 4-6 weeks. Following by DNA-extraction and then testing the samples by qPCR and LAMP techniques, researchers confirmed that the RG phytoplasma was detected at a higher titer than others, which indicates that RG phytoplasma is able to outcompete the SPLL and EY phytoplasmas [63, 66]. Additional strategies employed to combat phytoplasma diseases include rouging, which entails the prompt removal of diseased or infected plants once symptoms become evident (or as soon as phytoplasmas are identified through molecular detection methods) [74]. In addition, certification, which is a procedure where commercial production and nursery stocks undergo official regulation by competent government agencies for securing absence from phytoplasma diseases, can be used to prevent phytoplasma spread both within and between countries [74].
Growth and technological advances have immensely contributed to streamlining modern living. Almost every aspect of human life relies on the benefits of modern technology. The adoption of technology in the healthcare system is referred to as e-Health. According to Elharish et al [1], e-Health is the delivery of healthcare using modern electronic information and communication technologies. Healthcare services provided through electronic health include physical and psychological diagnosis and treatment, telepathology, vital sign monitoring, and teleconsultation, and the adoption of e-Health benefits healthcare practitioners and patients. Benefits of E-Health include saving time, reducing human errors, reducing healthcare costs, and giving patients insight into their health. The benefits of e-Health adoption have been seen in different regions worldwide. Despite the perceived benefits, developing countries show a go-slow in adopting e-Health. Prior studies explain the latter scenario from the funding and cost constraints perspective. However, other factors have contributed to the sustainable adoption of e-Health technology in developing countries. To facilitate swift and sustainable adoption of e-Health in developing countries, involved stakeholders should understand the connection between social, economic, and political factors challenging e-Health adoption in developing countries.
This research will expound the discussion on factors affecting the sustainable adoption of e-Health in developing countries using Syria as a case study. A meta-analysis of the current situation in Syria was conducted using online peer-reviewed databases such as Google Scholar, PMC, and PubMed. As mentioned earlier, the current study explains the slow adoption of e-Health in developing countries. The latter approach leaves many gaps in explaining the influence of social, political, and cultural factors impacting the adoption of e-Health in Syria. By addressing the research gap, the study will enhance the process of adapting e-Health in Syria and other developing countries. Sustainable adoption of e-Health requires a region to evaluate its capability and feasibility of the intended changes. However, external and internal factors within a jurisdiction compromise the latter moves. Developing the country’s economic, social, cultural, and organizational traits are among the most conspicuous factors affecting the sustainable adoption of e-Health. The situation in Syria is far worse than in many developing countries in the Middle East. The Syrian war has weakened the country’s ICT infrastructure, and the interplay between various cultural, economic, and war contributions has led to the unsustainable adoption of e-Health in Syria. Understanding factors compromising e-Health adoption in Syria gives the government a clear picture of evidence-based measures for improving its healthcare system.
The Syrian government has emphasized a decentralized healthcare system that focuses on providing primary healthcare at the village, district, and provincial levels. Irrespective of the measures embraced to streamline healthcare provision in Syria, the progressive wars in the region have seen a 60% decline in Syrian health care services. In addition to causing a decline in Syria`s population, the war in Syria is responsible for destroying healthcare infrastructure and, consequently, unsustainable adoption of e-Health. Medical facilities’ destruction has led to shortages of medications and medical supplies. In a report by the International Rescue Committee (IRC), Syria has a total of 507 hospitals (114 public hospitals and 393 private hospitals), which are distributed between cities unevenly. The latter statistics are grounded on attacks directed on healthcare facilities. According to Allah ham et al, (2022) [2]. Berlin-headquartered Syrian archive has documented videos of 412 separate attacks against a total of 270 medical facilities between 2011 and 2020. The progress of the Syrian war has increased healthcare disparities in the region, with an average of 706 persons per bed in 2020 compared to 734 persons per bed in 2011. The current situation in Syria requires immediate action, following that only 64% of hospitals and 52% of the region’s health care centers are functional [2]. Direct attacks on Syria`s health facilities and practitioners have seen a significant drop in healthcare practitioners. According to Karasapan (2016) [3], 70% of Syria’s healthcare providers have fled the country, with substantial cities experiencing mass migration of physicians. Aleppo, one of the major cities in Syrian, had 6000 physicians before the war, and by 2013 only 250 remained in the city. The deteriorating state of Syria`s health sector is also founded on reduced government spending on health as a percentage of GDP. According to Allahham et al, (2022) [2], Syria`s government spending on health reduced from 4.9% in 2005 to 3.4 % in 2010 and continued to reach less than half of the 2011 percentage.
Article Statement: The slow adoption of e-Health technology in developing countries is a multifaceted issue requiring responsible stakeholders to devise and resolve practical measures.
LITERATURE REVIEW
Lack of Awareness
The rate of technology acceptance varies with region and community members’ attitudes towards the technology. Cultural, economic, and social factors define innovation adoption rates resulting in five categories (innovators, early adopters, early majority, late majority, and laggards) of innovation [4]. Developed countries comprise early adopters and innovators. While innovators are motivated to accept trends in technology as soon as they emerge and appreciate technological changes, early adopters adopt new technology to achieve revolutionary changes and gain a competitive advantage. On the other hand, the early majority embrace technological changes to improve productivity. Syria and many developing countries fall into the laggards and late majority category. The latter categories are skeptical about innovative technology and are geared towards maintaining the current status quo. Cultural and organizational traits in Middle East countries explain the region’s unsustainable adoption of e-Health technology. Alajlani & Clarke [5] conducted case study research in Syria and Jordan to investigate cultural factors affecting the sustainable adoption of e-Health in the two regions. The study gathered data from key stakeholders in Syria and Jordan’s healthcare sector. Interviews and questionnaires were employed for a study population comprising 100 participants (50 from each country) and 45 professional participants (22 from Jordan and 23 from Syria). The study accessed the professional practitioners using face-to-face semi-structured interviews. The study aimed to investigate demographic traits in the two regions and identify factors likely to compromise e-Health adoption.
A thematic analysis revealed three interconnected themes; poor infrastructure, poor funding, and lack of technology training as significant factors leading to the slow adoption of e-Health. It was noted that Jordan was ahead of Syria in adopting e-Health. This was supported by the fact that Jordan started using e-Health technology way of Syria. Even though the two countries had problems funding e-Health programs, respondents from Syria did not perceive funding as a barrier to e-Health implementation [5]. Regardless of the noted difference, resistance from doctors and patients was a major factor affecting the sustainable development of e-Health. Lack of training and exposure to e-Health affected Syrian health professionals more than in Jordan. The latter findings align with the categories of innovators highlighted in the introduction. Syria falls in the laggard category of innovators, which explains why its health practitioners and patients display a go-slow in accepting e-Health.
Reform Challenges
Rapid development in information and communication technology requires community members and affected individuals to stipulate reforms in sectors affected by the changes. The innovation in e-Health creates an urge for health sectors to define structure and organizational changes. Attempts that are made to reform Middle East’s health sector have been met with notable problems that, in turn, lead to the slow adoption of technology. Al-Samarraie et al. [6] supported Alajlani & Clarke [5] with the arguments that Middle East’s go-slow in technology adoption results from stakeholders’ resistance. In a study to review progress in adopting and using telemedicine in Middle Eastern countries, Al-Samarraie et al. [6] conducted a literature review on 43 peer-reviewed articles published between 2010 and 2020. The research answered two questions “What is the current progress of adoption and use of telemedicine in the Middle East?” and “What are the key barriers to implementing telemedicine in the two countries?” Al-Samarraie et al. stated there are major cultural barriers affecting e-Health adoption in Middle Eastern countries include religious, traditional beliefs, literacy level, and linguistic barriers. The study also noted that the absence of laws and regulations to support the transformation process affected the sustainable adoption of e-Health. The legal and regulatory framework designed to guide the delivery of care in Syria shows that e-Health may compromise patients’ privacy, which eludes the nursing code of ethics. In addition to the reform challenges, other factors compromising the sustainable adoption of e-Health include organizational (poor training, media representation, insurance, and strategic planning), individual barriers, and poorly motivated healthcare workers.
Al-Samarraie et al, calculated the contribution of different factors in reduced rates of e-Health adoption in Syria as a percentage of the total number of barriers identified from the 43 peer-reviewed articles. The results showed that technological and organizational barriers are the most affecting factors.
Ay et al. [7] expanded on the factors affecting the sustainable adoption of e-Health by conducting cross-sectional, analytical, and observational studies. The study employed snowball sampling and structured questionnaires to collect data from the target population. A total of 196 surveys were carried out by a non-government organization in Jordan hosting Syrian refugees. Ay et al. findings align with both Alajlani & Clarke [5] and Al-Samarraie et al. [6] in that structural and social barriers limited the implementation of e-Health among Syrian refugees. The study’s findings provided insights to humanitarian organizations wishing to support Syria and other developing countries to adopt e-Health.
International intervention can facilitate the adoption of e-Health in Syrian. However, the government should evaluate its current situation to determine if the factors within its jurisdiction hinder the successful implementation of e-Health interventions. Granja, et al. [8] carried out a systematic review to evaluate the factors influencing the outcomes of e-Health intervention. The study found that e-Health intervention’s success depends on its perceived impacts on healthcare. According to Granja, et al [8], research on e-Health should be carried out before implementing the desired intervention. Even though Granja, et al did not directly contribute to Syria’s case study, they informed the research topic from the perspective of Syria’s current situation. Alajlani & Clarke [5] found that healthcare practitioners in Syria have the required awareness to support e-Health. The latter findings align with Granja, et al [8] whose finding indicates that research is a critical factor in defining the success of e-Health intervention. The fact that healthcare practitioners in Syria are not conversant with e-Health technology implies that they cannot explore e-Health. The overall impact is the unsustainable adoption of e-Health. The study also noted that the ICT barrier also challenges the sustainable implementation of e-Health in Syria.
Information Technology Barriers
Information and communication technology have been perceived as enablers of economic development. A notable discrepancy is, however, noted in developing countries whereby the poor are, in most cases, left out of enjoying the benefits of ICT. Touray, et al. [9] conducted a study to identify ICT barriers in literature and empirical findings and categorize the barriers into critical success factors. The study employed a systematic literature review and case study methodologies. The review analyzed 1107 articles published between 2000 and 2011, while the empirical data was collected through a total of 200 questionnaires to evaluate internet adoption at user levels. The achieved data were analyzed using open coding and non-hierarchical coding. The study found 43 ICT barriers using two different studies. Forty of the identified barriers were common in the two studies, while three arose from the empirical study findings. According to Touray, et al. [9], economic socio-culture (SC), economical (EC), infrastructure (IF), legal and regulatory (LR), technical (TN), and education skills (ED) compromised the adoption of e-Health in developing countries. The study concluded that politics and leadership and lack of internet exchange points are major barriers affecting e-Health adoption in developing countries.
Even though the study was not conducted in Middle Eastern countries, its findings align with the reports previously evaluated in this study. The three outstanding barriers affecting the adoption of e-Health in developing countries include lack of internet exchange points, interference from foreign governments, and micromanagement of e-Health.
Civil Conflicts
Regions with political instability and wars suffer numerous economic challenges that increase government spending on vital activities. Irrespective of the benefits of e-Health, the Syrian government has more stressed economic issues to handle from the ongoing war. In a study to evaluate the impacts of the Syrian war on the implementation of e-Health, Bowsher et al. [10] employed narrative hermeneutic methodology. The literature review included articles composed from 2000 onwards, whereas thematic analysis deduced common themes. According to Bowsher et al., altered security conditions in Syria require the healthcare sector to adopt and revise partial online training programs instead of focusing on in-person care delivery. The latter requirement does not align with the e-Health framework because e-Health offers in-person healthcare services. The role of e-Health in regions with political and civil instability is to expand and facilitate the delivery of care. It is, however, challenging that many regions with civil disruptions do not have the right resources to support the implementation of e-Health. Even though Bowsher et al. [10] have provided a detailed explanation of the effects of war on e-Health, their findings differ from previous findings [5-7]. The latter studies connected the poor adoption of e-Health in Syria to cultural, organizational, and social barriers. Bowsher et al. [10] explained the go-slow in e-Health adoption with arguments that conflicts require frequent changes in healthcare provision strategies, a move that requires plenty of resources. The scarcity of resources in Syria and many other developing nations makes it hard for the healthcare sector to adopt e-Health. However, Bowsher et al. agreed with previous studies that a lack of professional training also compromises the adoption of e-Health in Syria.
Factors affecting clinician adoption of mobile health tools
Clinician’s attitude towards a healthcare innovation plays a critical role in defining the success or failure of the healthcare innovation. Jacob, et al. [11] article reported the findings of a structured review article to explore the relevance of published studies regarding social, organizational, and technological factors compromising the adoption of e-Health in developing countries. The study evaluated 171 peer-reviewed articles from MEDLINE, PubMed, SAGE, and Cochrane online databases. Technological factors defining clinicians’ adoption of e-health include outdated systems, system errors, poor quality outcomes, and data security issues [11]. Even though technological barriers are crucial in hindering the sustainable adoption of e-Health, workflow-related factors arose as the main factor from the contacted literature. The world is witnessing a notable shortage of healthcare workers. This implies that nurses and other health care practitioners have tight fixtures to attend to, which leaves them no time to invest in advancing their technological skills. The situation in developing countries is worse because, apart from the shortage of healthcare providers, the region does not have enough resources to invest in continuous nurses training programs. Even though Jacob et al. concentrated on identifying physician-related factors, their findings relate to most of the articles contacted earlier in this review. For instance, technological factors identified in [5,8,9] are also highlighted in Jacob, et al study [11].
Decrease in physician-to-patient ratio
According to World Bank Report (2015) [12], the physician-to-patient ratio has been decreasing tremendously since the onset of the Syrian war. For instance, Syria’s physician-to-patient ratio has been declining since the onset of the war, from 1:370 to a current ratio of 1:546. Stephan [13] supported the latter ideology with findings that 30% to 60% of Syrian physicians have left their country.
Challenges in the adoption processes of e-Health
Zayyad & Toycan [14] highlighted how adopting e-Health technology in developing countries is crucial in managing healthcare facilities while ensuring they offer quality services to patients. They used a modified technology acceptance model (TAM) to highlight how to facilitate the implementation of electronic health records (EHR), and the reasons why the process should be undertaken in phases. However, as the facilitator, the Syrian government should bring the reality check to the table and display why the new EHR system benefits the health sector and healthcare dispensation. In this context, the impediment factors from different stakeholders in the sector should be handled at the initial stages to ensure a smooth transition. In essence, the most important factor that should be considered is how the communication, practicability, and implementation of the EHR system are supposed to be embraced by all the stakeholders involved because they will be vital in running the technological system.
Using the narrative hermeneutic methodology, Alajlani & Clarke [5] found five qualities that should be handled before the diffusion of innovation and invention of new technologies in any healthcare setting, and these adaptations help to ensure the success of the procedure. Individual attitudes also play a critical role in this process of adopting new technologies, and due to that reason, people are concerned with five qualities. These include relative advantage: where the individuals adopting the new innovation must see how it will improve the old ways of doing things. In addressing this issue, Syrian healthcare professionals are supposed to be taken through the way that the accessibility and the availability of patient information under the new system will reduce the time unless when they were using the old system. The latter findings were supported by Said [15], who used Egypt’s healthcare to highlight how under EHR, the patient’s past and current medical information are accessible with a single click and input of the relevant data. This will ensure that they can be assisted faster during an emergency because different healthcare professionals can view their medical history under one platform.
Learning Measures for Improving e-Health
Matlin et al. [16] used qualitative research methods to highlight the Syrian government’s role in the EHR system implementation to improve healthcare safety, efficiency, and quality, especially during the refugee crisis. Furthermore, the government is supposed to guarantee that it protects the patient’s privacy and personal rights as it is envisioned under the law. Namatovu & Semwanga [17], supported the latter study’s finding with qualitative research to learn how the process of presenting the EHR system compromises its adoption in Syria. The reason for their involvement is that they will be responsible for training the individuals who will take part in the final phase of inputting the patient’s information into the new system. Syria is a religious and conservative country that follows Islamic laws and principles, and it is vital to use these approaches to ensure civic education is available for all the people involved. Therefore, the transition from the traditional form of handling patient information is supposed to be put into the new system, and it should be carried out with utmost responsibility and care to avoid errors and misuse of the new data.
Shawahna [18] used CDSS systems research to indicate how the efficacy and quality delivery of Syrian and other Middle East countries healthcare in both rural and urban areas rely on communication, interaction, and association with various care providers, medical residents, physicians, nurses, and other interested parties in the medical field. Therefore, when the different stakeholders converge for the meeting, they should be made to understand that the change in the EHR system does not only impact them; it is a collective responsibility of all the other parties with whom they interact daily. The transition to electronic health records (EHR) is not an easy task for any health center or for the physicians, the hospital management, the members of staff, and the nurses who are usually at the center of these changes because they make the transition to become easier [17]. The essence of converging healthcare providers and other stakeholders is to ensure that they can understand the importance and significance of having operational electronic health records (EHR) and how it will change their lives.
In the initial process of implementing electronic health records (EHR), all interested parties should be called to stakeholder meetings to be enlightened and educated on their role in the procedure. The meetings should be frequently held during the initial stages to ensure that all parties comply with all the issues they are taught, and they should continue until everyone is conversant with what the EHR entails. The type of information nurses should start with the basic process of how the EHR system works from an outsider’s perspective, the security measures that are put in place to avoid third-party interferences, and the implications that should occur when the nurses breach those terms and conditions [19]. The legal procedures entailed in the EHR system are made in such a manner that they are supposed to be agreed upon by all parties through consent because of the private and personal information they hold. In this context, it means that before the whole EHR process is started, in-house communication, coordination, and planning are supposed to be laid out before implementation.
Significance of e-Health compatibility
Zayyad and Toycan [14] indicate how electronic health and technology should be compatible with the new system while advancing values and practices that ensure the innovation aligns with the healthcare practices of the state or government. In this context, healthcare professionals are supposed to know that the inclusion of technology in how healthcare services are undertaken is a concept meant to infuse the old methods into a new platform. The old information will only be input into the EHR, and no other changes will be initiated because the data in the old system will just be keyed in for easy accessibility. Namatovu & Semwanga [17] supported the earlier applications of e-Health by noting that the simplicity factor should also be part of the new EHR system so healthcare professionals can easily operate the new technology. Based on these analogies, they highlighted how adopters must believe they can easily master the new technology; because if they consider it difficult, the greater the resistance. Therefore, it is the duty of the management and the trainers to use the simplest way possible to ensure that all involved personnel will master the system within a specified time span.
Hossain et al. [20] conducted a study in rural Bangladesh using the TAM model to learn how the trial-ability of the new EHR system should be made before the whole process is fully implemented. The report of Salminen & Mursu [9] also supports this approach, where the trial period should show that all the parties involved in operating EHR can “play around’ with the new technology while exploring its capabilities. The trial period of any new technology comes with the chance for the adopters to make mistakes so that they can be rectified and changed to a simpler version, if any, is available. Hossain, et al [20] used 292 respondents where through the trials; the seriousness of resisting change by the adopters indicated that new technology could be learned with an open mind. Observable results: the adopter should have adequate evidence, information, and data on how the new EHR has succeeded in other situations. Most of the data and information should highlight EHR’s success, especially in bigger health centers that have included technology in all their services and their rate of offering quality services to their patients. Therefore, when the smaller healthcare centers adapt to the new changes, it is only meant to ensure that they are not left out when the whole system changes, and they familiarize themselves with technology in all their healthcare delivery [10]. In all these adaptations, it will help the nurses to have an open mind that when they advance in their careers, the bigger health centers are also using the technology, and therefore, it is essential for them to learn on a low-level scale before they are enrolled in other complex EHR systems.
Summary findings:
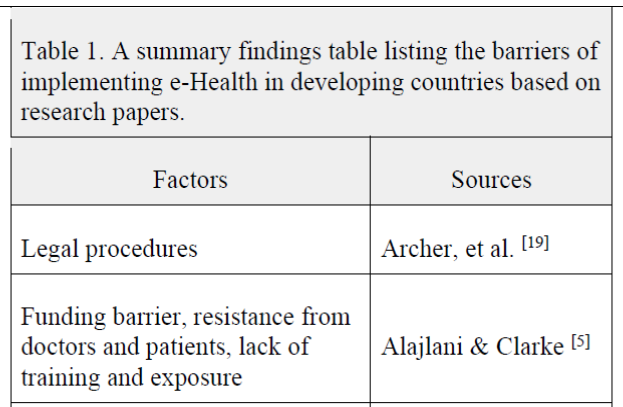
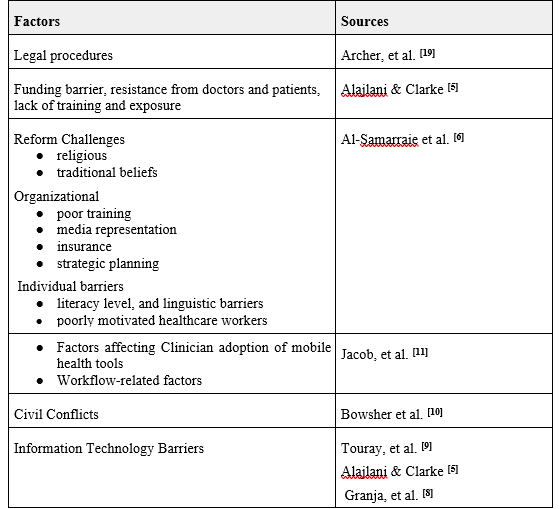
By providing a clear and concise summary of the key findings from the literature, Table 1 could help to inform decision-making, guide the development of interventions and policies, and identify areas for future research.
Table 1. A summary findings table listing the barriers of implementing e-Health in developing countries based on research papers.
CONCLUSION
Electronic health is among the most promising trends in healthcare. Implementing e-Health is associated with many benefits to the healthcare department and other stakeholders in the healthcare docket. Irrespective of the benefits of e-Health, developing countries are lagging behind in its adoption. Using a case study of Syria, this article has identified some major challenges compromising the sustainable adoption of e-Health in developing countries. The most conspicuous challenge affecting arose from the lack of training and exposure to e-Health affected Syrian health professionals more than in Jordan [5]. Additionally, cultural barriers (religious, traditional beliefs, literacy level, and linguistic barriers) also compromised the sustainable adoption of e-Health [9]. The ongoing war in Syria negatively affected the implementation of e-Health since the government does not have adequate resources to facilitate the implementation process. Altered security conditions in Syria require the healthcare sector to adopt and revise partial online training programs instead of focusing on in-person care delivery. The latter requirement does not align with the e-Health framework because e-Health offers in-person healthcare services. In summary, the unsustainable adoption of e-Health in Syrian and other developing countries can be classified into three categories that, include social, systematic, economic, and organizational barriers.
RECOMMENDATION
Improving e-Health adoption in Syria and other developing countries is indeed crucial for advancing healthcare services and ensuring better access to medical facilities. Implementing effective measures to increase the consumption of e-Health requires a multi-faceted approach. We here list several proposed strategies:
Continuous Training for Healthcare Practitioners
Subjecting healthcare practitioners to continuous training on emerging technologies is an excellent step. It will equip them with the necessary skills and knowledge to effectively use e-Health tools and technologies in their practice. This approach helps address the issue of brain drain, where physicians leave the country in search of better opportunities abroad. By offering up-to-date training, the country can retain skilled professionals and attract others who want to work in a technologically advanced healthcare environment.
Investing in Modern Technology
Investing in modern technology is essential for upgrading healthcare facilities and providing healthcare practitioners with the tools they need to adopt e-Health practices. This could include providing hospitals and clinics with the necessary infrastructure, such as electronic health record systems, telemedicine platforms, and remote monitoring devices. By making these technologies available, healthcare practitioners can become more familiar with and embrace e-Health solutions.
Learning from Jordan’s Experience
Drawing insights from Jordan’s experience can be beneficial. As Jordan introduced e-Health technology earlier, it can serve as a valuable case study for Syria to understand the benefits, challenges, and best practices in implementing e-Health initiatives. This information can guide Syria in making informed decisions and avoiding potential pitfalls in its e-Health adoption process.
Addressing Cultural and Systemic Barriers
Cultural and systemic barriers can impede the successful adoption of e-Health in Syria. To overcome these challenges, investing in community-based education programs is essential. These programs should focus on educating healthcare practitioners and community members about the advantages of e-Health and dispelling any misconceptions or fears related to its implementation. By involving the community in the process, acceptance and support for e-Health initiatives can be significantly improved.
Encouraging E-Health Research
With a growing adoption of e-Health practices, there is an opportunity for Syria to invest in e-Health research. Research in this field can help identify areas for improvement, measure the impact of e-Health technologies on patient outcomes and healthcare costs, and refine the implementation strategies for better results.
Collaboration with International Partners
Syria can also benefit from collaborating with international partners and organizations experienced in e-Health adoption. These collaborations can provide technical expertise, financial support, and access to best practices, helping Syria leapfrog some challenges and accelerate its e-Health transformation.
In summary, enhancing e-Health adoption in Syria requires a comprehensive approach that includes continuous training for healthcare practitioners, investment in modern technology, learning from other countries’ experiences, addressing cultural and systemic barriers through community-based education, encouraging research, and fostering international collaboration. By implementing these strategies, Syria can pave the way for more efficient and effective healthcare delivery through e-Health solutions.
Due to rapid industrialization, urbanization, and population growth, the demand for energy and its resources is increasing annually. It is projected that global energy consumption will reach 812 quadrillion KJ in 2035, meanwhile, fossil fuels are still the dominant energy source. The use of petroleum and other liquid fossil fuels worldwide was 85.7 million barrels/day in 2008 and is expected to increase to 112.2 million barrels/day in 2035 (1). It is expected that we will deplete the entire global oil reserve by 2050 (2). Approximately 86% of global CO2 emission is associated with the use of fossil fuels with 2 billion tons year-1 discharged by coal-fired power plants as prevalent around the globe (3,4). Due to concerns over rising fuel prices, declining reserves of fossil fuels, and environmental issues such as pollution and global warming, a novel, sustainable approach to energy production is urgently needed. Biomass and fuels derived from its processing are one of promising alternatives to conventional fossil fuels (5). Sustainability, feedstock diversity, and low to no emissions of gasses such as soot, SO2, or NOx make biomass a promising energy source. However, treatment is needed for biomass to be converted into biofuels and chemicals that have ready use due to its high moisture and oxygen content and consequently lower energy-density compared to fossil fuels (6,7). According to Faaij (2006) research, bio-energy could meet current global energy needs with a potential of over 1000 EJ year-1(8). Additionally, biofuels are carbon neutral as the CO2 released by their combustion is consumed again for the growth of other biomass via photosynthesis (1). Fig. 1 shows the conversion routes of biomass to bioenergy. Biogas, ethanol and biodiesel are examples of first-generation biofuels that are directly tied to biomass that is frequently edible (9–13). To make first-generation bioethanol, only a few distinct feedstocks are actually employed, namely sugarcane or corn. Brazil is one of the top countries using sugarcane as a feedstock for the manufacture of biofuels.
Fig. 1 Conversion of biomass to bioenergy
In the future, efficiency can be further improved through the development of superior crop varieties, improved crop management techniques, and advancements in ethanol production processes (8). The only other biofuel made on an industrial basis is biodiesel produced from oily plants and seeds and commonly used in Europe and Asia (14). There is a number of environmental and socioeconomic concerns around the first generation biofuels future perspective such as land use, food competitivness, and lifecycle (15). Moreover, the growth is dictated by biomass prices on the market. Some of these challenges are banished through newer generation fuels. Second generation biofuels utilize the range of different feedstocks such as non-edible lignocelulosic biomass, different residues and waste products such as bio-waste and municipal solid waste (14,16).
Thermochemical conversion
The most well-known method of converting biogenic waste is thermochemical conversion, which also includes pyrolysis, gasification, liquefaction, hydropyrolysis, and reforming (17–21). The biomass is transformed into hydrocarbons and synthesis gas through gasification, whereas pyrolysis and liquefaction directly transform the biomass at high temperatures into bio-oils, gases, and char.
Hydrothermal process
Energy-denser product is derived from biomass via hydrothemal conversion.As the technology operates in an aques environment, no pre-drying of the feedstock is necessery and biomass with higher moisture content can be directly utilized (22). HTC yields solid fuel (hydrochar) under temperatures between 180–280 for 5–240 min (23). From 250°C to 375°C and pressure of 10–25 MPa HTL takes place producing bio-crude or crude-oil,which is a liquid fuel consisting of insoluable organics (24,25). Bio-crude requires only slight upgrading to be used commercially while by-products of liquifaction have lucrative applications (i.e. fertilizer). Possible future research areas include setting up a plant suitable for both wet and dry feedstock, analyzing the influence of various parameters, optimizing for better conversion, and developing theoretical models to accurately represent the process depending on the feedstock (26). Moreover, When biomass is heated to high temperatures during hydrothermal liquefaction above 375°C the process is known as HTG, macromolecules are broken down into molecules with smaller molecular weights, creating syngas see Fig.2
Fig.2 Hydrothermal process
Torrefaction
Torrefaction is a thermal conversion process used to pre-treat biomass converting it into a more uniform and energy dense product. Heating under inert atmosphere in the temperature range of 200-300°C enhances the fuel properties of biomass by improving combustion properties (27), homogenuity, physical and chemical properties making it similar to coal.The torrefied biomass is biologically stable, hydrophobic, and significantly lower in moisture content compared to raw feedstocks (28). It is expected that all traditional pelletisation facilities would transition to torreaction plants for the production of torrefied pellets. Furthermore, the biomass pre-treated like this is easier to handle and transport to locations where it can be applied for heating fuel, cofiring, gassification, etc. Optimisation of this technology is expected around combustor, heat exhangers, as well as nitrogen feed, while research is being conducted on techno-economical performance of the technology (7).
Pyrolysis
For the waste reduction of biomass conversion technologies entire carbon content of the feedstock should be converted into a valuable product (29). Pyrolysis distributes carbon atoms between biocrude, char, and syngas (30). Despite major success of recent engineering endovours on this topic (31), further research should be conducated on novel reactors with improved cost and overall effectiveness. Furthermore, intergeration with anaerobic digestion is a promissing future direction for higher quality bio-oil and solution of an environmental problem (29).
Gasification and biofuels
Gasification produces less toxic fuels compared to fossil that can use existing infrastructure. While commercial production of biofuels from gasification does not currently exist, there has been increasing interest and research on this approach over the past few decades. The gasification process produces syngas, a mixture of carbon monoxide and hydrogen, from biomass. This syngas then undergoes further chemical processing to produce fuels and chemicals that are readily available on the market as shown in Fig.3.
Fig. 3 Scheme of biofuels production through gasification
Through methanation synthesis gas is produced. FTS yields kerosene (jet fuel), disel, and gasoline liquid fuels. Several commercial-scale initiatives are currently in the works, especially in the United States but also in Europe and Japan, even though bio-FT is currently in the demonstration stage. The initiatives cover a wide range of end products and feedstock options. Even carbon capture and storage will be used in one project, the Bayou Fuels biorefinery in the United States, to create negative emissions, sometimes referred to as carbon dioxide reduction. Biojet kerosene has to make significant strides in order to align with the Net Zero Scenario by 2030. The success of biojet kerosene depends on reducing costs, implementing clear regulatory schemes and policies, and diversifying sustainable feedstock supplies beyond waste and edible oils. Synthesized methanol can be further upgraded into gasoline, DME (fuel additive), and polymers, as well as acetic acid and formaldehyde. Hydrogen that is produced in gasification process can be used directly as a fuel or to further synthesize ammonia and urea (8,32). According to IEA, these production pathways could enable renewable diesel and biojet kerosene to sustainably scale up to the levels necessary in the Net Zero Scenario as they utilize more abundant feedstock compared to some already commercially viable options such as HVO and HEFA (32). The equipment needed for these secondary processes is similar to that used for natural gas, but gas cleaning is more intensive. There have been some pilot projects demonstrating this approach, but technological challenges remain compared to other biofuel production methods. While current process technologies can be applied once clean syngas is available, further research and development are needed to improve gas-cleaning, scale up processes, and achieve higher efficiencies and lower costs through more advanced concepts like liquid phase methanol production and improved gas separation. Some countries are increasing interest and investment in research on advanced gasification for syngas production as a long-term strategy.
Hybrid Renewable System Technology
Another initiative to tackle energy challenges in a sustainable way is to adopt hybrid renewable energy systems. Such a setting that combines multiple renewable energy sources overcomes the issue of spatiotemporal variability of these resources. Compared to single resource-based energy generation systems, integrated renewable energy systems can increase energy storage capacity, reduce energy production costs, and improve the quality of generated power (33). Furthermore, such systems offer greater flexibility and promote overall socio-economic growth (34,35). Hybrid renewable systems incorporating thermal conversion of biomass with other renewable energy sources received considerable attention in research (35–39). For instance, Facchinetti et al. worked on the integration of a solid fuel cell-gas turbine cycle powered with hydrothermally converted biomass obtaining the efficiency of 63% (40). Heidari et al. performed hydrothermal carbonization of biomass. The hydrochar was used in the integrated system to produce power and process water in anaerobic digestion to obtain biogas later used as a gaseous fuel (41). On the other hand, biomass can be anaerobically digested to produce biogas that can be used to generate heat or electricity, while the digestate can be pyrolyzed in the integrated system to obtain gas, oil, and char. Deng at al. found that such a system could be self-sustaining by combusting pyrolytic gas and excess char. Another important aspect is the energy storage (42). Concepts such as Green to Green energy system aim to find a green storage system, such as fuel cell, for the green energy (43,44). Lin et al. proposed a plant for simultaneous generation of electricity and liquid hydrogen involving a lignocellulosic biomass gasification-integrated gas turbine and hydrogen liquefaction cycle with an electrolyzer process (45). Table 1 gives an overview of what other initiatives were taken on thermal conversion technology hybrid systems. However, study by Lee at al. showed that more research should be done on testing conceptually created models in real life conditions, addressing power fluctuation issues in the grid-connected system, removal of ash and moisture via pre-treatment technologies, etc (33).
Table 1: An overview of systems integrating thermochemical conversion of biomass with other renewable energy technologies
Feedstock
System setting
Aim
Source
Lignocellulosic biomass
Gasification concentrated solar thermal power
Electricity generation
(46)
Fusion power gasification
Hydrocarbon fuel or hydrogen production
(47)
Adiabatic compressed air energy storage gasification
Electricity generation and energy storage
(48)
Bio-oil combustion – photovoltaics
Electricity generation
(49)
Anaerobic digestion – pyrolysis
Electricity generation and pyrolytic product production
(50)
Gasification – pyrolysis
Biochar production and electricity generation
(51)
Biomass combustion – biomass gasification – biomass pyrolysis photovoltaics – wind power vanadium redox battery-based energy storage system
Seaweed/wood
Pyrolysis – anaerobic digestion
Methane production
(42)
Wheat straw
Anaerobic digestion hydrothermal carbonization
Energy recovery
(52)
Spent coffee ground
Hydrothermal carbonization – anaerobic digestion
Methane production
(41)
Carbon capture and storage
IPCC’s Fourth Assessment Report highlighted that emissions must be diminished by 50-85% until 2050 to keep global warming below 2°C. Through IPCC’s Special Renewable Energy Sources and Climate Change Mitigation and Technology Roadmap Carbon Capture and Storage in Industrial Applications, bio-CCS was recognized as a single wide-reaching technology that could reach negative carbon footprint (53–55). It combines sustainable biomass conversion with CO2 Capture and Storage technology. For its growth, biomass absorbs CO2 from the atmosphere. Nevertheless, in conversion processes, CO2 is once more exhausted in the air. CCS technology aims to capture this exhaustion, deliver, and store it safely underground through natural mechanisms (residual, dissolution, and mineral trapping)(15).
The production of biofuels, such as ethanol fermentation and bio-FT, produces a high concentration of CO2 as a byproduct. As a result, these pathways have the potential to capture and utilize CO2 for storage or use. The cost of capture and transport is relatively low. Due to the high concentration of CO2 produced, no additional purification is required apart from dehydration. Once the CO2 is captured, it can be compressed and transported via pipeline, truck, or ship to a storage site or be used in some way. For example, captured CO2 has been sold for use in enhanced oil recovery or within the food and beverage sector. Researchers are exploring the potential of combining fossil fuels with sustainably grown biomass in flexible conversion facilities to produce fuels and other products. Gasification-based conversion platforms offer a flexible method for fuel production from biomass, coal, and natural gas. Combining sustainably grown biomass with (partial) CO2 capture allows for overall negative CO2 emissions per unit of energy produced on a life cycle basis. This approach can be used to produce hydrogen, where all carbon monoxide produced is shifted to hydrogen and CO2. A co-feeding strategy, such as with coal, can be attractive in the short term for organizing large-scale biomass supplies. When equipped with CO2 capture facilities, the input share of fossil fuel can still become “carbon neutral”. Negative emissions could be obtained by using more biomass. For instance, bio-CSS can be applied in large industrial operations where there is a local heat or power requirement, particularly in industrial clusters where CCS infrastructure can be shared. The use of biomass in the industry to replace fossil fuels has a variety of potential applications, including small and medium-scale heat and power, fuel substitution in cement kilns, and injection in blast furnace steel and iron-making. Existing large-scale gasification technology can be used to gasify biomass feedstock, which could be supplied as crude bio-oils obtained via pyrolysis or treated via torrefaction, reducing transport costs and facilitating feeding to pressurized gasification systems. Some exploratory work on large-scale and long-distance biomass supplies for large-scale syngas production has been done with promising results, indicating that this is a concept that deserves further study and development. European Technology Platform for Zero Emission Fossil Fuel Power Plants shows that an additional step further could be made by completely substituting fossil fuels and using bio-CSS in an independent bio-fuel production plant. Biomass is converted to char and gas in the gasifier. Char amounts for 6% of overall carbon content of the biomass. After gas treating, 52% of carbon content can be stored in CO2, while the remaining 42% are converted through FT- synthesis (15).
Conclusion
This review discusses the future of biomass conversion as a sustainable approach to energy production and carbon emissions reduction. It is an abundant and sustainable resource with the potential to reduce or entirely substitute fossil fuels. We explore different types of biofuels and conversion technologis specifically thermal conversion. Gasification is a promissing process to convert biomass into non-toxic fuels and useful chemicals while using existing infrastructure. For it to be applied on the industrial scale, further research on advanced tehniques is needed to improve gas cleaning and lower the costs of highly effective processes. Hybrid renewable energy systems incorporating thermochemical conversion are promising direction to tackle climate change and simultaniously overcome energy challenges in certain regions. However, more work should be done on the ways to maximize renewable sources fraction while minimizing the costs, real life testing, etc. Furthermore, carbon capture and storage technology combined with sustainable biofuels production could help achieve carbon negativity. International agencies such as IEA and UNIDO are highlighting the importance of scaling up such technologies in the near future and need for additional research in this direction so that Net Zero goals can be achieved.
Journal:Syrian Journal for Science and Innovation Abbreviation: SJSI Publisher: Higher Commission for Scientific Research Address of Publisher: Syria – Damascus – Seven Square ISSN – Online: 2959-8591 Publishing Frequency: Quartal Launched Year: 2023 This journal is licensed under a:Creative Commons Attribution 4.0 International License.
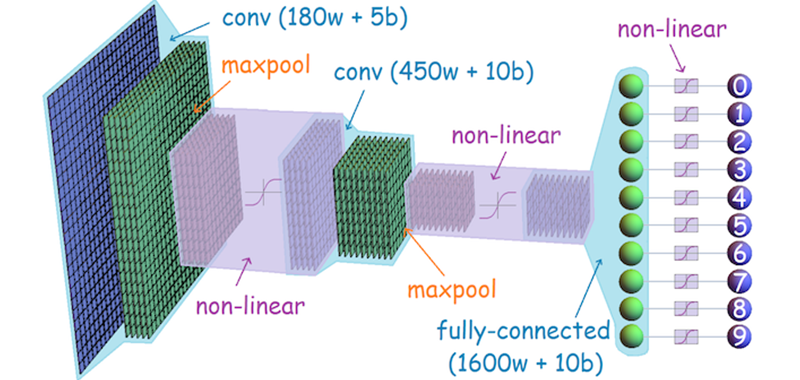
![Figure 2: CAPE network architecture [9]](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F2-1-300x93.png)
![Figure 3: ClothCap approach [28]](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F3-300x192.png)
![Figure 4: Displacement maps with a UV parametrization to represent surface geometry [25]](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F4-300x53.png)
![Figure 5: Inria Dataset approach [14]](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F5.png)
![Figure 6: Qualitative pose estimation results on BUFF dataset [15] Left to right: scan, Yang et al. [27], BUFF result](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F6-214x300.png)
![Figure 7: Annotations of the 3D People Dataset [10]](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F7-300x81.png)
![Figure 8: CAPE model for clothed humans [9]](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F8-300x100.png)
![Figure 9: Qualitative results on fashion images [9]SMPL [8] results are shown in green, CAPE results are in blue](https://journal.hcsr.gov.sy/wp-content/uploads/2024/06/F9-300x249.png)

![Figure 1 Electron microscopy picture (6000x) of a cross section of sieve tubes with phytoplasmas, modified from [8].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/1-9-300x199.png)

![Figure 3 Symptoms of Elm yellows phytoplasma on infected Ulmus americana showing yellowing leaves and epinasty compared with a healthy plant on the left side in the picture, modified from [32].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/1-11-300x252.png)

![Figure 5 Depicts olive trees affected by phytoplasmas, showing shortened internodes, witches'-brooms, and smaller leaves (a), as well as hypertrophied inflorescences (b). This image has been adapted from [32].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/1-13-e1701086953493-300x129.png)
![Figure 6 The life cycle of phytoplasmas is depicted with phytoplasmas represented as red dots. It commences with 'Acquisition Feeding,' during which an insect, like a leafhopper, acquires phytoplasmas while feeding. Following this, a 'Latency Period' ensues, indicating the time it takes for the phytoplasmas to reach an infection titer, necessary for their transmission. The final stage is 'Infection Feeding,' during which the insect transmits phytoplasmas to healthy plants as it feeds, modified from [37].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/2-300x199.jpg)
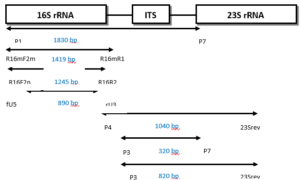
![Figure 8 How the SYBR GREEN assay works step by step, modified from [56].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/1-16-259x300.png)
![Figure 9 How Taqman assays work step by step, modified from [61].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/2-1-260x300.jpg)

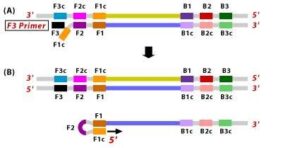



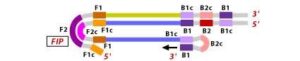
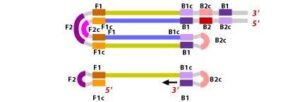
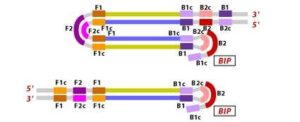
![Figure 10 Illustration depicting the operational principle of LAMP assays, involving a set of six primers that consist of external primers (F3 and B3), internal primers (FIP and BIP), and loop primers (loopF and loopB), modified from [64].](https://journal.hcsr.gov.sy/wp-content/uploads/2023/11/2-9-300x92.jpg)