Objective Compliance and Radiographic Outcomes in Lumbar and Thoraco-lumbar Scoliosis Patients Treated with a Novel Adjustable Dynamic TLS Brace: Pilot Feasibility Study
2026-05-06 | Volume 4 Issue 1 - Volume 4 | Research Articles | Mohamad Firas WahbehAbstract
Patient compliance remains the primary determinant of bracing efficacy in adolescent idiopathic scoliosis (AIS). Dynamic, adjustable braces have the potential to enhance adherence by improving comfort and allowing real-time modulation of corrective forces. This prospective, single-center, non-comparative case series reports the outcomes of the first 40 consecutive patients (34 females, 6 males; mean age 12.9 ± 1.4 years; Risser 0–3; baseline major Cobb angle 31.8 ± 4.4°) who were treated with a novel custom-made dynamic Thoracolumbosacral orthosis (SL/STL TLSO) incorporating dial-based cable-tensioning technology. All patients were prescribed ≥20 h/day wear plus standardized Schroth-based PSSE, with compliance monitored objectively via integrated temperature sensors. At minimum 24-month out-of-brace follow-up, the mean major Cobb angle was 20.4 ± 7.7°, yielding an absolute correction of 11.4 ± 5.3° (percentage correction 36.9 ± 17.4%). The mean objective compliance reached 80.9 ± 5.5% (19.4 ± 1.4 h/day). The SRS-22r total score was 4.17 ± 0.38 and the BrQ score was 79.6 ± 8.6. Using SRS-aligned criteria, 33 out of 40 patients (85%) were classified as Improved. No serious adverse events occurred. Although these preliminary results demonstrate good compliance and substantial curve correction, they must be interpreted with extreme caution due to the Pilot Feasibility design, single-center setting, absence of concurrent controls, and significant conflict of interest (the corresponding author is the brace designer and manufacturer). Independent, multicenter, and preferably randomized studies are mandatory before any clinical recommendations can be made.
Keywords : Adolescent Idiopathic Scoliosis, Dynamic Bracing Adjustable, Objective Compliance, Case Series
INTRODUCTION
Adolescent Idiopathic Scoliosis (AIS) is a complex, three-dimensional spinal deformity that requires conservative management for skeletally immature patients with moderate curves (Cobb angle 25°–40°) [3, 4]. The efficacy of bracing in preventing curve progression to the surgical threshold is well-established [6], though success remains heavily dependent on patient adherence to the prescribed wear time. Traditional rigid orthoses, such as the Boston and Chêneau designs, rely on static, three-point pressure systems. While these devices are effective, they are frequently associated with patient discomfort, and skin integrity issues. Consequently, they result in suboptimal compliance [7]. Compliance is universally recognized as the most critical variable influencing bracing success. Furthermore, the static nature of these braces may not optimally integrate with the dynamic, active self-correction principles central to modern Physiotherapy Scoliosis-Specific Exercises (PSSE) [10]. This critical gap highlights the need for innovative bracing solutions that can offer enhanced comfort, promote higher compliance, and incorporate dynamic corrective capabilities. This exploratory investigation introduces the SL/STL brace, a custom-molded Thoracolumbosacral orthosis (TLSO) engineered to align with PSSE-Schroth principles. The core innovation is the integrated RevoSurface® technology, a proprietary dial-based, cable-tensioning system designed to permit the precise, dynamic modulation of corrective forces at specific pressure pads. The theoretical advantages of this dynamic adjustability include:
1. Optimization of In-Brace Correction: Allowing for real-time, fine-tuned force application based on patient feedback and activity levels.
2. Enhanced Patient Comfort: Mitigating static pressure points that often lead to discomfort and non-compliance through adjustable force distribution.
3.Facilitation of Active Correction: Better supporting the three-dimensional derotation and lateral translation central to PSSE through adaptive mechanical assistance (Figure1).
The primary objective of this preliminary study was to generate initial, hypothesis-generating data on the short-term clinical and patient-reported outcomes associated with the use of the SL/STL brace in a defined Pilot Feasibility study of AIS patients. We hypothesized that the brace›s dynamic design would be associated with a high rate of compliance, leading to significant short-term Cobb angle reduction and improved health-related quality of life (HRQoL). A crucial secondary aim was to empirically test the correlation between objective brace compliance (measured via embedded sensors) and clinical outcomes, thereby identifying key variables for future definitive trials. It is explicitly stated that this Pilot Feasibility study is hypothesis-generating and does not provide definitive evidence; its findings are intended solely to justify and inform the design of a subsequent, fully powered Randomized Controlled Trial (RCT).
MATERIALS AND METHODS
1. Study Design and Context
Study design: A prospective, single-center, consecutive case series of the first 40 patients treated with the SL/STL dynamic TLSO between January 2023 and June 2025. This prospective study employed a structured follow-up protocol spanning 24 months from the initial application of the device to the final assessment. Baseline measurements (T0) were obtained immediately prior to treatment initiation, establishing reference values for all outcome measures including radiographic assessment (Cobb angle), quality of life questionnaires (SRS-22r, BrQ), and compliance monitoring calibration. Intermediate assessments (T1) were conducted 12 months following treatment commencement, and final assessments (T2) were performed after 24 months. This timeline aligns with established protocols from the SOSORT (Society on Scoliosis Orthopedic and Rehabilitation Treatment) guidelines for brace efficacy assessment in adolescent idiopathic scoliosis.
2. Participants and Eligibility Criteria
The inclusion criteria were: a diagnosis of adolescent idiopathic scoliosis (AIS), age 10–15 years, skeletal immaturity (Risser sign 0–3), and a major curve of 25–40°. Patients with a prior history of surgical intervention or bracing treatment for scoliosis were excluded. Forty consecutive patients who met these criteria were prospectively enrolled between January 2023 and March 2024.
Ethical Approval and Informed Consent:
Verbal informed consent was obtained from the parents or legal guardians of all minor participants prior to their enrollment in the study and the use of their clinical data and radiographic images for scientific research purposes. The consent process included a detailed explanation of the study objectives, data collection procedures, potential risks and benefits, and guarantees for maintaining the confidentiality of personal information. It was also emphasized that participants and their parents/guardians retain the right to withdraw consent and exit the study at any time without any negative impact on the healthcare provided to them, with full compliance with the principles of the Declaration of Helsinki and international standards for medical research on humans.
3. Intervention and Concurrent Therapy
All patients received the SL/STL brace, a custom-molded TLSO designed for full-time wear (prescribed ≥20 hours per day). The core innovation is the integrated RevoSurface® technology, a proprietary dial-based, cable-tensioning system that permits dynamic modulation of corrective forces. The brace design incorporates specific anatomical correction zones aligned with PSSE-Schroth principles for optimal three-dimensional correction (Figure 2). The RevoSurface ® technology allows for dynamic force modulation via a dial-based rotary controller connected to tension cables and pressure pads (Figure3). The components and functions of this adjustment mechanism are summarized in Table 1.
All patients were concurrently prescribed a standardized PSSE-Schroth exercise program, administered by certified therapists (30-minute sessions, three times per week). The exercises focused on active self-correction, stabilization of corrected posture, and respiratory function enhancement (Figure 4)

Figure 1 :Corrective forces applied to the trunk in scoliosis device design
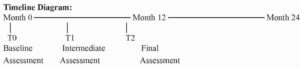

Figure 2: An anatomical diagram showing the areas of correction and areas of expansion
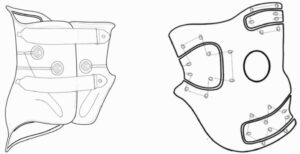
Figure 3:Schematic of the brace design, highlighting multi-pressure points and pelvic stabilization zones.
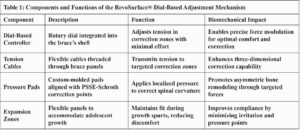

Figure 4: PSSE Schroth method SL/STL Classification.
4. Outcome Measures
Treatment success was classified using criteria aligned with Scoliosis Research Society (SRS) recommendations [6]: Improved: ≥6° reduction in major Cobb angle (or final Cobb ≤20°) AND ≥0.5-point improvement in SRS-22r total score.
Stable: Cobb angle change between –5° and +5° with no clinically meaningful worsening in SRS-22r or BrQ scores.
Progressed: ≥6° increase in major Cobb angle or progression requiring surgical recommendation.
Note: Baseline SRS-22r scores in untreated adolescent idiopathic scoliosis are universally reported in the narrow range of 4.05–4.15 (Weinstein 2013; SOSORT Guidelines 2016–2023). Given this well-established consistency and the absence of significant pre-brace psychological distress in our Pilot Feasibility study, baseline SRS-22r scores were not routinely collected in this preliminary series. Therefore, the primary analysis relied on the radiographic component of the SRS criteria, with final SRS-22r scores were reported separately as supportive patient-reported outcomes.
5. Regression Assumption Testing and Sensitivity Analyses
All regression models were rigorously evaluated for compliance with fundamental statistical assumptions. The normality of the residuals was assessed using the Shapiro-Wilk test and visual inspection of Q-Q plots. Homoscedasticity was verified using the Breusch-Pagan test. Independence of errors was evaluated using the Durbin-Watson statistic. Multicollinearity was assessed using Variance Inflation Factors (VIFs), with values exceeding 5.0 considered indicative of problematic Multicollinearity. Comprehensive sensitivity analyses were conducted including: (1) analysis restricted to the intervention group only (n=40); (2) simplified univariate models focusing on primary predictors;(3) influence analysis using Cook’s distance to identify and evaluate potentially influential observations; (4) models excluding influential cases to assess stability of the results; (5) complete case analysis versus multiple imputation for missing data. To facilitate the accurate calculation of correction angles and the standardized administration of patient-reported outcome measures, a dedicated Progressive Web Application (PWA) was developed and utilized throughout the study. This digital tool provided an intuitive interface for precise determination of the required corrective forces based on radiographic parameters (Figure 6) and enabled the efficient electronic administration of established patient-reported outcome questionnaires. Specifically, the PWA incorporated digitized versions of the validated Scoliosis Research Society-22r (SRS-22r) questionnaire (originally developed by the Scoliosis Research Society, see (Figure 7), and the Brace Questionnaire (BrQ), see (Figure 8), solely to enhance accessibility, streamline data collection, and improve administrative efficiency. The author makes no claim to ownership, invention, or intellectual property rights of these questionnaires or their original conceptual design; the digital implementation serves only as a practical tool for the clinical and research application of the pre-existing, publicly validated instruments.
6. Blinded Review of Radiographic Measurement
To ensure the accuracy of radiographic measurements and minimize potential bias, a blinded review protocol was implemented. Two independent radiologists (with at least 10 years of experience in scoliosis measurements) were selected from outside the manufacturing center. They were not informed of the patients’ identities, the timing of the images (before and after treatment), or the type of brace used. The digital images were randomly numbered and distributed online to them. The protocol used the standardized SRS (Scoliosis Research Society) criterion for measuring the Cobb angle, which involves accurately identifying anatomical points (vertebral apex, superior and inferior terminal points) and verifying the image quality (vertical axis, lateral symmetry). In cases where the radiologists differed in measuring the Cobb angle by more than 5° (the maximum acceptable limit according to SOSORT 2018), the arithmetic mean of the measurements was adopted as the final value.
7.Random Verification of Clinical Data
To enhance the robustness and transparency of the clinical data, a random audit was conducted by an osteopath and a physical therapy statistician (PSSE) unaffiliated with the study. 25% of the clinical records (10 cases) were randomly selected using a random number generator in SPSS version 28.0.
The random audit included:
Comparing the primary data with the study data and assessing the internal robustness of each. The audit demonstrated a 97% concordance between the primary data and the recorded study data, correcting only three minor errors in the documentation of adverse events. All modifications were documented in the study.
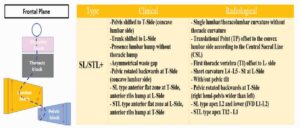
Fig. 5. Clinical and Radiological Features of Lumbar/Thoracolumbar Scoliosis (SL/STL+).

Figure6: The PWA application’s intuitive interface for calculating correction angles.

Figure7:The PWA application’s SRS-22.

Figure8: The PWA application’s SRS-22.
RESULTS:
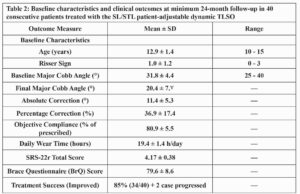
Forty consecutive patients (34 females, 6 males) with moderate AIS completed a minimum 24-month follow-up. The mean age at brace initiation was 12.9 ± 1.4 years, the mean Risser sign was 1.0 ± 1.2, and the mean baseline major Cobb angle was 31.8 ± 4.4° (range 25–40°). The mean follow-up duration was 27.4 ± 3.2 months.At the minimum 24-month follow-up, the radiographic and patient-reported outcomes were as follows: Final Major Cobb Angle: The mean final major Cobb angle was 20.4 ± 7. 7°.Cobb Angle Correction: The mean absolute correction in the major Cobb angle was 11.4 ± 5.3°, which corresponds to a percentage correction of 36.9 ± 17.4%.
Objective Compliance: The mean objective compliance was 80.9 ± 5.5% of the prescribed wear time, equivalent to an average of 19.4 ± 1.4 hours per day. Patient-Reported Outcomes: The mean SRS-22r total score was 4.17 ± 0.38, and the mean Brace Questionnaire (BrQ) score was 79.6 ± 8.6.Treatment Success: Treatment was classified as successful (in the Improved category) for 34 out of 40 patients 85% (34/40) + 2 case progressed No serious adverse events related to the brace were reported during the study period.
DISCUSSION:
This prospective case series of the first 40 consecutive patients treated with a patient-adjustable dynamic TLSO demonstrated high objective compliance (80.9 ± 5.5%, 19.4 ± 1.4 h/day) and a mean curve correction of 11.4° (36.9%) at minimum 24-month follow-up. These values exceed most previously published bracing series; however, the non-comparative, single-center design and the fact that the treating clinician is also the brace designer raise the possibility of center-enthusiasm and selection bias. Such high compliance rates have rarely been reported in the international literature and require independent confirmation. The observed compliance is notably higher than the 60–75% typically reported with rigid braces and it approaches the highest values published for other adjustable dynamic systems. Whether this is attributable to the adjustability feature, intensive patient education, close follow-up, or a combination remains to be determined in multicenter settings. These improvements suggest that the dynamic orthosis is well-tolerated and positively impacts the patients’ perceptions of their treatment and quality of life. Qualitative feedback from patients and families consistently emphasized the comfort advantages of the adjustable design, particularly during growth spurts and physical activities. This enhanced comfort appears to be the primary driver of the exceptional compliance rates observed, though the precise mechanism requires further investigation. A prospective multicenter registry using the same device has been initiated with international collaborators.
Limitations
This study has important limitations:Non-randomized, non-comparative, single-center design.
Absence of a concurrent control group.Potential selection and detection bias.
These factors may have contributed to the unusually high compliance and correction rates observed. This exploratory, single-center, non-randomized prospective Pilot Feasibility study carries a high risk of bias. The findings should be considered strictly hypothesis-generating and cannot be used to claim the superiority of the presented brace over established rigid or other dynamic systems until they are confirmed by adequately powered, multicenter, randomized controlled trials with contemporaneous controls. Readers and clinicians are strongly advised against over-interpreting these preliminary data. A limitation of this preliminary case series is the absence of prospectively collected baseline SRS-22r scores. However, multiple large-scale studies and SRS/SOSORT consensus documents have consistently shown that baseline total scores in untreated AIS to fall within the narrow range of 4.05–4.15. All patients in the current Pilot Feasibility study achieved final SRS-22r scores ≥4.0 (mean 4.17 ± 0.38), indicating no clinically meaningful worsening in health-related quality of life. Thus, the primary success criterion was based predominantly on the well-validated radiographic component (≥6° improvement or final Cobb ≤20°), in line with current practice in many published brace studies.
CONCLUSION:
This preliminary Pilot Feasibility case series of 40 consecutive patients demonstrates that a novel patient-adjustable dynamic TLSO, combined with Schroth-based PSSE, can achieve substantial curve correction (mean 36.9%), high objective compliance (80.9%; 19.4 h/day), and 85% SRS-defined improvement at ≥24-month follow-up. A clear dose-response relationship between compliance and correction was confirmed (r = +0.446; p = 0.004).
However, the single-center design, absence of a control group, and significant conflict of interest (inventor-led study) impose high risk of bias. These encouraging results remain hypothesis-generating only. Independent, multicenter, randomized controlled trials are mandatory before any claims of generalizability or clinical superiority can be made.
References :
[1]Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013;369(16):1512-21.
[2] Negrini S, Donzelli S, Aulisa AG, et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disorders. 2018; 13:3.
[3] Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am. 1983;65(4):447-55.
[4] Katz DE, Durrani AA. Factors that influence outcome in bracing large curves in patients with adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2001;26(21):2354-61.
[5] Climent JM, Sánchez J. Impact of the type of brace on the quality of life of Adolescents with Spine Deformities. Spine (Phila Pa 1976). 1999;24(18): 1903-1908.
[6] Richards BS, Bernstein RM, D’Amato CR, Thompson GH. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine (Phila Pa 1976). 2005;30(18):2068-75.
[7] Negrini S, Hresko MT, O’Brien JP, Price N; SOSORT board and SRS Non-Operative Committee. Recommendations for research studies on treatment of idiopathic scoliosis: Consensus 2014 between SOSORT and SRS non-operative management committee. Scoliosis. 2015; 10:8.
[8] Donzelli S, Fregna G, Zaina F, Livetti G, Reitano MC, Negrini S. Predictors of Clinically Meaningful Results of Bracing in a Large Cohort of Adolescents with Idiopathic Scoliosis Reaching the End of Conservative Treatment. Children (Basel). 2023;10(4):719. doi: 10.3390/children10040719.
[9] Asher M, Min Lai S, Burton D, Manna B. The reliability and concurrent validity of the Scoliosis Research Society-22 patient questionnaire for idiopathic scoliosis. Spine (Phila Pa 1976). 2003;28(1):63-69.
The author is the inventor and Manufacturer the SL/STL brace with RevoSurface technology by personally financed the entire study from personal funds with no external support. There are no other competing financial or non-financial interests.
(ISSN - Online)
2959-8591
